The analgesic triad: Managing patient pain from oral disease
Veterinary patients with chronic oral disease requiring oral surgery benefit tremendously from what I call the analgesic triad: continuous rate infusions (CRIs), physiologically targeted post-operative analgesics and regional nerve blocks.
Veterinary patients with chronic oral disease requiring oral surgery benefit tremendously from what I call the analgesic triad: continuous rate infusions (CRIs), physiologically targeted post-operative analgesics and regional nerve blocks. Each component complements the other two, maximizing pre- and post-operative patient comfort and intraoperative safety, and aids the knowledgeable practitioner in safely managing surgical patients with chronic oral pain.
Painful or not?
Veterinary patients with chronic oral disease often do not demonstrate clinical signs attributable to oral pain. This is unfortunate, because patients often suffer for extended periods of time before abnormalities are noticed and addressed. Even more unfortunate is the fact that many pets with chronic oral disease never receive care either because of pet owners' lack of compliance or failure to notice. In my experience, the vast majority of patients do not present for oral pain. Postoperatively, however, the patient whose oral disease is surgically eliminated will demonstrate positive signs consistent with pain resolution. Pet owners consistently and overwhelmingly report behavioral changes consistent with a healthier pet. These include greater appetite, increased activity, playful behavior and a return to oral manipulation of toys or chews.
Client education
Awareness of the behavioral changes above is crucial in client education. The majority of patients won't demonstrate pain that pet owners can recognize during an initial client education discussion. Use these first discussions immediately following recognition of the pet's existing disease as an opportunity for education.
The most common oral condition in which pain is an occult component is periodontal disease. Client education is paramount to achieving compliance. Inflammation and odor indicate infection. Cleaning the patients' teeth does little to solve the underlying periodontal infection. We must stress to clients that we are treating infection rather than cleaning teeth. Pictures can be used to demonstrate what hides beneath the gum line causing pain (Photos 1 and 2).



Photo 1: Images like these can be used for client education to demonstrate pain below the gumline. Without dental radiography, this patient likely would just have had teeth cleaned, and the true pathology below the gumline would have been missed.
CRIs and post-operative analgesics
Many practitioners already recognize the importance of treating chronic oral pain and currently use the chronic pain analgesic triad. CRIs target various mechanisms of pain generation and perpetuation and are used pre-operatively and continued variably into the post-operative period. Post-operative pain management administered by clients should provide continued coverage using similar compounds targeting the same mechanisms. While a discussion of the pathophysiology of pain is beyond the scope of this manuscript, three primary components represent the targets of CRI and home-based client-administered pain management. These include central sensitization alteration (wind-up), opiate-receptor activation and peripheral inflammation attenuation.


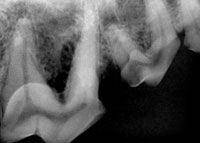
Photo 2: Radiographically severe bone loss in the furcation of the right maxillary fourth premolar is present. This patient was noticeably more active Âfollowing extraction.
Wind-up. Patients with chronic oral pain benefit from analgesics that decrease the effect of proalgesic mediators within the modulation center of the brainstem. Glutamate and substance P are two such compounds that act in concert to allow exaggerated pain impulses to reach the higher brain centers resulting in pain perception. CRI use with compounds that alter this effect block the NMDA receptors that allow pain signals to reach perception. Ketamine is commonly used to modulate pain signals within the brainstem by blocking the NMDA receptor. Lidocaine has been shown to act centrally to decrease central sensitization and is used in the CRI regimen in dogs. Doses and calculations can be done with a free spreadsheet available online at www.vasg.org.
Peripheral sensitization. Peripheral inflammatory mediators play a major role in generation and perpetuation of chronic oral pain conditions in pets. Host-mediated pro-inflammatory cytokines and chemokines are mobilized at the diseased site from host cells in response to bacterial antigens. Peripheral sensitization is initiated when compounds like histamine result in vasodilation, allowing these proalgesic mediators to extend to previously non-inflamed tissue. Alteration of this effect is achieved by decreasing the production of some of these substances by using NSAIDs to dampen host response.
Opiate-receptor activation. The brain attempts to counter the number and intensity of pain signals reaching the higher centers by initiating the production of internal opiates?— endorphins, dynorphins and enkephalins — to occupy opiate receptors on nerves, bone, gingiva and other cell types. Unfortunately, these do not produce adequate analgesia in many chronic pain states. Use of synthetic opiates including morphine, fentanyl and hydromorphone in CRI and client-administered home care bridges the therapeutic gap left by the descending inhibitory opiates.
Intraoperative physiologic benefits. Not only does CRI initiate the desired goals of altering wind-up, decreasing inflammation and stimulating opiate receptors, it also decreases the amount of inhalant anesthetic needed during the intraoperative period. Maximizing this effect with the addition of complete sodium channel blockade ensures that ascending sensory signals are eliminated. This is accomplished by using regional nerve blocks.
Regional nerve blocks
Rounding out the triad, regional nerve blocks should be employed to eliminate cortical sensory perception generated by surgical manipulation of tooth, bone or soft tissue. The four blocks used in mesocephalic and dolichocephalic dogs are the rostral and caudal maxillary, and the rostral and caudal mandibular.



Photo 3: Due to the short infraorbital canal in cats and brachycepalic dogs, the rostral maxillary (infraorbital) block delivers the agent adjacent to the pterygopalatine and infraorbital nerves to block the entire quadrant including palatal bone and mucosa.
Only three blocks are required in cats and brachycephalic dogs. The rostral maxillary (infraorbital) block provides complete quadrant blockade in these animals due to their short infraorbital canal (Photo 3). The caudal mandibular (inferior alveolar, mandibular alveolar) block has been associated with severe tongue trauma in rare instances (Photo 4). This occurs in the immediate postoperative period and can be avoided by manually placing the tongue in a normal intraoral position and visually monitoring the patient until it can maintain sternal recumbency.



Photo 4: The caudal mandibular (inferior alveolar, mandibular alveolar) block has been implicated in the induction of tongue trauma. Proper patient monitoring during recovery can totally eliminate this rare problem.
Taking advantage of regional nerve blocks allows blood pressure, cardiac output and respiration rate to approximate levels expected in patients not experiencing surgical tissue manipulation. Tissue oxygenation and perfusion are positively affected, making it easier to avoid hypothermia. Properly administered regional nerve blocks allow the patient to wake up pain free, provide smoother recoveries and minimize or eliminate the immediate need for additional postoperative analgesics. Proper planning provides for the other components of the triad to be on board when regional block efficacy wanes.
Summary
Chronic pain pathophysiology is extremely complex. This "analgesic triad" for patients with chronic oral pain simplifies the approach to pain management while spanning the scope of the major mechanisms involved in pain generation and perpetuation.
Dr. Beckman is acting president of the American Veterinary Dental Society and owns a dentistry and oral surgery practice in Punta Gorda, Fla. He sees referrals at Affiliated Veterinary Specialists in Orlando and at Georgia Veterinary Specialists in Atlanta, lectures internationally and operates the Veterinary Dental Education Center in Punta Gorda.













