Imaging techniques for the pancreas (Proceedings)
Pancreatitis is a common consideration in dogs and in an increasing number of cats presented for vomiting, anorexia, lethargy, or abdominal pain.
Introduction
Pancreatitis is a common consideration in dogs and in an increasing number of cats presented for vomiting, anorexia, lethargy, or abdominal pain. The disease however, is difficult to diagnose definitively, especially in cats. Clinicopathologic data, including amylase and lipase values are used routinely when canine pancreatitis is suspected. However, they may be normal, or elevated from other disease processes. They are not useful in cats. Newer tests, including canine and feline PLI are being used with increasing frequency, and are now commercially available. They appear to be fairly sensitive for pancreatits, but results are not available for several days. Imaging techniques have become an essential part of the workup in patients suspected of having pancreatitis.
Radiology of the pancreas
The normal canine pancreas is not seen on abdominal radiographs. However, in cats, the left pancreatic limb can often be seen as a thin linear soft tissue opacity extending to the left, between the gastric fundus, cranial pole of the left kidney, and spleen.
Both acute and chronic pancreatitis, as well as pancreatic neoplasia can result in changes visible on survey abdominal radiographs. Potential radiographic signs include:
1. Loss of abdominal detail, primarily in the right cranial abdomen, due to focal peritonitis
2. Mass effect in the right cranial abdomen
3. Displacement of the pylorus cranially, or to the left
4. Ventral or right sided displacement of the descending duodenum
5. Caudal displacement of the transverse colon
6. Bowel loops adjacent to the pancreas (usually duodenum) may be gas-filled (ileus), or corrugated/spastic in appearance


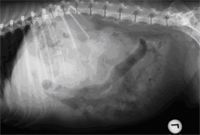
Lateral abdominal radiograph of a dog with pancreatitis. There is a mass effect in the cranial abdomen, caudal to the stomach, as well as ventral displacement of the gas-filled descending duodenum.
Radiographs are frequently normal in dogs and cats with pancreatitis. In a previous study, only 24% (10/70 cases) of dogs with acute pancreatitis had radiographic changes consistent with this disease. Computed tomography is a sensitive means of making a diagnosis of pancreatitis or pancreatic neoplasia in people, but has limited availability, is expensive, and requires general anesthesia in veterinary medicine. Ultrasound, therefore, has become the imaging modality of choice in the diagnosis of pancreatic disease. Ultrasound examination of the pancreas can be difficult, however. The canine pancreas, unlike the liver or spleen, is often not seen as a discrete organ, and therefore the pancreatic region and its anatomic landmarks must be examined. The pancreas is surrounded by gas filled structures, including the duodenum, stomach, and colon, which may obscure visualization. Finally, abdominal pain in patients with pancreatitis may prevent the firm pressure on the transducer needed to visualize the pancreatic area.
Ultrasound of the pancreas
Canine
The canine pancreas has an echogenicity similar to surrounding fat, and does not have a well defined capsule. Because it is not usually visualized as a discrete organ, the sonographer must be familiar with the anatomy and anatomic landmarks used to identify the pancreatic region. The use of a higher frequency transducer will aid in visualization of pancreatic tissue. The pancreas is divided into left and right lobes which are joined together at the pancreatic body. The right pancreatic lobe lies dorsomedial to the duodenum, ventral to the right kidney, and lateral to the portal vein. The cranial and caudal pancreaticoduodenal veins course through the right lobe, parallel to the descending duodenum. The right lobe may be imaged by scanning longitudinally along the right lateral abdomen, using the descending duodenum and right kidney as landmarks. The descending duodenum can be visualized ventral and either lateral or medial to the right kidney, as the largest diameter small intestinal loop, and one which follows the straightest course longitudinally down the right body wall. The right lobe of the pancreas lies dorsomedial to the descending duodenum. The pancreaticoduodenal vein is frequently visualized undulating somewhat parallel to the descending duodenum. The descending duodenum should be followed caudally until it turns medially and becomes the ascending duodenum. Cross-sectional images of the duodenum are very helpful (and preferred by the author) in imaging the pancreas (located dorsomedial to the cross section of the duodenum). In large or deep chested dogs, a lateral intercostal approach may be needed. Using a right lateral transverse view through the 10-12th intercostal space, the right pancreatic lobe will be located ventral to the right kidney, ventrolateral to the portal vein, and dorsomedial or dorsal to the descending duodenum.



Cross sectional image of the descending duodenum. The right limb of the pancreas is located dorsal and medial to the duodenum, and is slightly hypoechoic to surrounding tissue
The pancreatic body joins the two lobes and is located immediately ventral to the portal vein and cranioventral to the right kidney. The body lies caudal to the pyloric region.
The left pancreatic lobe may be more difficult to visualize due to surrounding gas-filled structures (stomach and colon). It may be located in a triangular region cranial to the left kidney, caudal to the stomach, and medial to the spleen in the left cranial abdomen. It lies caudo-dorsal to the stomach and craniodorsal to the transverse colon.
The normal canine pancreas may on occasion be visualized, especially when using high frequency (7-10 MHz) transducers. It appears slightly more echogenic than the liver, and slightly less than the spleen.
Feline
Unlike the pancreas in the dog, the feline pancreas is typically visible as a discrete organ on ultrasound examination. It appears as a hypoechoic (similar to liver echogenicity) linear, well marginated organ immediately caudal to the stomach. The pancreatic duct extends through the center of the pancreas, visualized as a well demarcated anechoic tubular structure. In fact, visualization of the pancreatic duct is sometimes key to locating the pancreas. The pancreatico-duodenal vein, often prominent in the dog, is usually not seen
The right limb of the feline pancreas is small and less routinely visualized, but is located dorsomedial to the descending duodenum. The body and left limb of the feline pancreas are more consistently imaged, especially if using higher frequency transducers (7MHz or higher). The pancreatic body is identified directly caudal to the pylorus-duodenal angle, medial to the proximal duodenum, and ventral to the portal vein. The left limb can be identified caudal to the stomach, cranial to the left kidney, and medial to the spleen. In an imaging plane parallel to and adjacent to the left costal arch, the longitudinal image of the left limb may be followed laterally to the spleen.
Normal dimensions of the pancreas and pancreatic duct have been reported in the cat. Normal ranges for pancreatic body and left limb width are 0.3-1.0 cm, with a mean of approximately 5mm. Pancreatic duct diameter ranges from 0.7-2.5mm, with a mean of about 1mm. There is a slight increase in pancreatic duct diameter with increasing age.

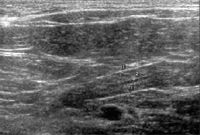
Ultrasound image of the left pancreatic limb in a cat. Calipers (#1) outline the thickness of the pancreas. Calipers #2 outline the diameter of the pancreatic duct.
Abnormal appearance
Pancreatitis: canine
Inflammation, edema, necrosis, and hemorrhage associated with acute pancreatitis result in an enlarged, irregular, hypoechoic pancreas. The affected areas may be diffuse, or patchy and poorly defined. The surrounding omental fat is usually hyperechoic secondary to saponification. Other associated changes occur in the descending duodenum, which can appear thickened, dilated and fluid-filled (ileus), or corrugated secondary to duodenitis. Pancreatitis is the most common cause of extrahepatic biliary obstruction in the dog, and can result in dilation of the gall bladder and common bile duct. Focal peritoneal effusion often accompanies acute pancreatitis. The right lobe seems to be the most commonly affected portion of the pancreas with acute disease, but this may simply be because it is more easily imaged than the left lobe. Chronic, low grade, or resolving pancreatitis appears as a slightly more echogenic pancreas with better defined, smooth borders. Associated changes such as hyperechoic peripancreatic fat, duodenitis, and abdominal effusion usually are absent.


Ultrasound image of a dog with pancreatitis. The duodenum is irregular (corrugated). The inflamed, hypoechoic pancreas (P) is located dorsal to the duodenum, and is surrounded by hyperechoic fat.
Pancreatitis: feline
The sensitivity of ultrasound alone for the diagnosis of feline pancreatitis is low. Acute necrotizing pancreatitis may result in an enlarged (thickened), hypoechoic pancreas with irregular margins. The surrounding mesentery may become hyperechoic due to fat saponification. The duodenum may become thickened or corrugated, or appear atonic and fluid-filled. Focal peritoneal fluid may also occur. However, these changes may not be present in every case (low sensitivity, high specificity). The ultrasound appearance of chronic pancreatitis is less well defined, and may be identical to those seen in acute necrotizing pancreatitis, with the exception of duodenal and adjacent omental fat changes. Fibrosis and atrophy, likely representing end stage chronic pancreatitis, may result in decreased width of the pancreas. Pancreatic duct dilation has been reported in pancreatitis. However, pancreatic duct dilation is more likely a normal aging change in the cat. Severe pancreatic duct dilation has been reported with duct obstruction.


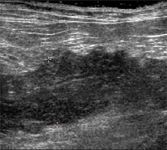
Longitudinal ultrasound image of the left pancreatic limb of a cat with pancreatitis. The pancreas is thickened (2.0 cm between calipers), hypoechoic, and irregular.
Pancreatic pseudocyst
Pancreatic pseudocysts are focal collections of pancreatic enzymes, blood, and products of tissue digestion within the pancreas. Eventually, a thick fibrous or granulation tissue capsule forms around the fluid collection. Pseudocysts are associated with acute pancreatitis, but require several weeks to develop. If small (less than 4 cm), they may resolve on their own. Larger or persistent (more than 6 weeks) pseudocysts require surgical drainage or removal. On ultrasound examination, they appear generally hypoechoic or anechoic, may have acoustic enhancement, and usually contain echogenic debris. Often, they are surrounded by a thick wall. It is difficult to differentiate a pancreatic pseudocyst from a pancreatic abscess on ultrasound exam alone. A needle aspirate may be required for a definitive diagnosis. One report of percutaneous ultrasound guided drainage of a pancreatic pseudocyst resulted in gradual resolution of the cyst. Complications of a persistent untreated pseudocyst include secondary infections, rupture, and hemorrhage.
Pancreatic abscess
Abscesses are collections of purulent material and necrotic tissue within the pancreas or extending into adjacent tissues. Pancreatic abscesses develop from secondary infection of necrotic pancreatic tissue, and are a serious complication of acute pancreatitis. They are often fatal unless there is surgical intervention. It is difficult to differentiate between pancreatic abscesses, pseudocysts, and even neoplastic disease. Abscesses may appear as ill defined mass lesions within the pancreas, containing both hypoechoic and hyperechoic areas. A thick or poorly defined wall may surround the abscess. These changes are similar to pseudocysts and tumors, so a needle aspirate or surgical biopsy is needed for a definitive diagnosis.
Pancreatic nodular hyperplasia
Nodular hyperplasia of the pancreas appears to be common in older cats and dogs, and is likely not clinically significant. Hypoechoic nodules distributed diffusely within normal pancreatic parenchyma may be seen as an incidental finding on ultrasound examination. However, nodular hyperplasia cannot be differentiated from malignant pancreatic neoplasia, which can appear similar on ultrasound examination. A biopsy is need for a definitive diagnosis.
Pancreatic neoplasia
Insulinomas (islet cell tumors) are suspected in some animals with hypoglycemia. These tumors generally are small (about 1 cm), focal, hypoechoic nodules which may be located in any part of the pancreas. Because they are easily missed, a negative ultrasound exam should not rule out insulinomas. Metastatic lesions in adjacent lymph nodes or liver may be more reliably imaged.
Pancreatic carcinomas are a differential for any mass lesion within the pancreas. However, ultrasound cannot reliably differentiate neplasia from pancreatitis, pseudocyst, abscess or nodular hyperplasia. A focal mass is probably the most common ultrasound appearance for malignant neoplasia. In cats, it has been reported that the only ultrasound feature unique to malignant pancreatic neoplasia (versus nodular hyperplasia) is the presence of a single mass greater than 2.0cm in at least one dimension. In this study, feline pancreatic neoplasias tended to have a single, larger mass lesion, while nodular hyperplasia tended to have multiple, smaller nodules. However, there is considerable overlap of both ultrasound and radiographic findings, requiring cytology or histopathology for a definitive diagnosis.














Veterinary scene down under: Australia welcomes first mobile CT scanner, and more news
June 25th 2024Updates on the launch of the first mobile CT scanner available for Australian pets; and learn about the innovative device which simplifies placement of urinary catheters in female dogs
Read More


