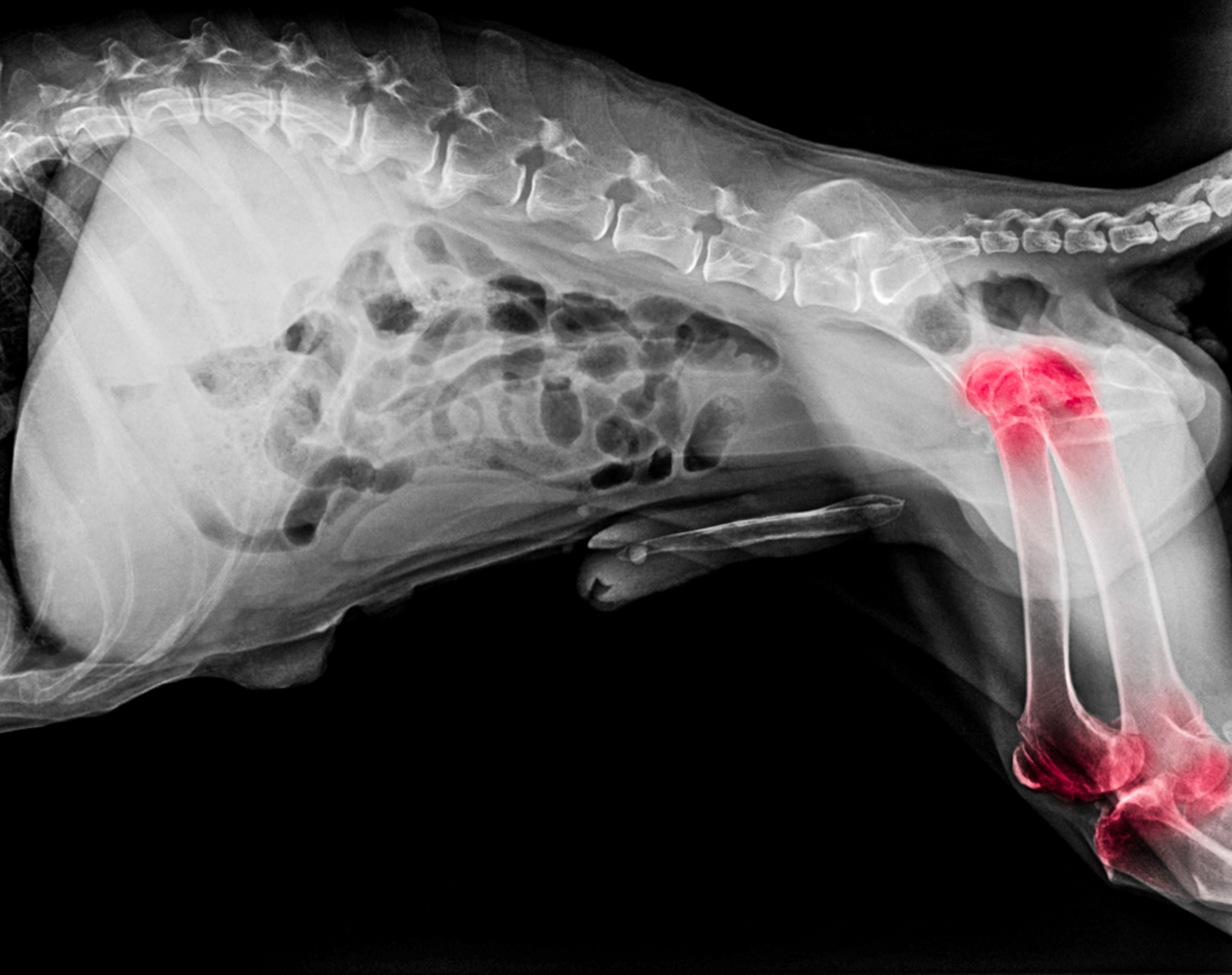
Considering osteoarthritic disease at any age
Mobility problems in younger dogs may be linked to the condition often seen in older pets


kintarapong / stock.adobe.com
When we look at an old dog with decreased mobility, we think of osteoarthritis (OA), but delegating the problem to that life stage can be misleading. In fact, although we certainly see the incidence and impact of OA increasing as dogs get older, for the most part this is a secondary condition to orthopedic issues that likely happened when the patient was younger.
Many developmental orthopedic diseases have their start in young dogs, including hip and elbow dysplasia, osteochondrosis, patellar luxation, and avascular necrosis of the femoral head. Add injuries to the list such as those of the cranial cruciate ligament, and appropriate management from the initiating point is essential.
Also, the size of the animal matters. Not only are larger dogs and breeds predisposed to dysplasia, but obesity plays a large role in OA. Certainly, the size and extra weight can place undue stress on already compromised joints, but the pro-inflammatory aspects of adipose tissue contribute to the overall systemic chronic inflammation that exacerbates chronic pain and aging. Maintaining an ideal weight is critical.
Every practitioner is likely well educated about the impact of chronic or maladaptive pain, with central plasticity and sensitization, and the vicious cycle of inflammatory components and markers. Signs may be subtle at first, so assessment of mobility and posture can start with an educated owner and continue in the clinic with gait analysis, radiographs, and palpation. Sometimes, it is challenging to localize specific pain and it can be helpful to use devices such as a thermal imaging tool and even a wearable monitor that can quantify acute and chronic pain by measuring direct pain biosignals (PainTrace; BioTraceIT).
Drug therapies
Dealing with OA is management, not just treatment, though nonsteroidal anti-inflammatory drugs (NSAIDs) are still the foundation for these conditions. Exploring multimodal approaches may lead to adding other components or substitution for NSAIDs, if necessary.
Amantadine (Gocovri; Supernus Pharmaceuticals) is an N-methyl-D-aspartate inhibitor that you can start at 3 to 5 mg/kg once daily then increase to twice daily if the liver is healthy. Gabapentin is frequently added in to treatment plans, though we do not know the mode of action and additional research would be optimal. With a wide range of doses that we can increase over time (around 10 mg/kg up to 3 times daily), many patients seem to have benefited from this drug, but always taper off gradually.
Since few dogs can metabolize tramadol to its active molecule, it is not as effective as we once hoped. It works in cats but try to give that bitter medication on a regular basis. Cats with OA now have better options with the monoclonal antibody frunevetmab (Solensia; Zoetis) by inhibiting nerve growth factor that causes pain originating within the spinal cord.
Supplements
Since most supplements can be added to food or given as a tasty treat, this is an easy “fix,” but the science isn’t always there and the full list of components and products is astounding. The most evidence is available for omega-3 fatty acids, added to diets or given as a supplement. Ideally, 100 mg EPA+DHA/ kg of lean body weight is a dog’s dose, and 50 to 60 mg/kg for cats, but do not overdose and count the calories. There is less evidence for glucosamine/ chondroitin sulfate (and all combinations), but clinical experience may support their use as part of the OA management plan. Sticking to products from reputable companies that have supporting literature and quality control is recommended.
Although we still have a lot to learn about cannabidiol supplements from the hemp plant, there is some evidence to suggest there are anti-inflammatory benefits. Again, stick with reputable companies in the veterinary field.
Early interventions
If conditions are recognized and diagnosed at earlier stages, any preemptive actions to minimize long-term changes can be beneficial. Surgery for some, including excision (femoral head and neck osteotomy), arthrodesis, arthroplasty, and joint replacement, may be indicated. Earlier use of disease-modifying OA drugs such as polysulfated glycosaminoglycan or pentosan polysulfate sodium, which is not available in US, can begin to slow the progression of cartilage damage. These products can also be used in older patients with osteoarthritis.
Additional therapies may include intra-articular injections of corticosteroids, hyaluronic acid, platelet-rich plasma and stem cells. These injections take training and can be technique sensitive, but results can be rewarding.
Physical therapy may include hands-on manipulation with passive joint movement, massage, acupuncture, and thermal and cryotherapy. Exercise at its simplest can help build muscle strength and improve the range of motion of joints with appropriate levels for the individual. More intense physical therapy with rehabilitation exercises can provide site-specific strength, mobility, and pain modulation.
Physical devices can also improve a patient’s comfort levels, including electrical stimulation (such as a unit for transcutaneous electrical nerve stimulation) that can help improve joint mobility and circulatory drainage. Targeted pulsed electromagnetic field (tPEMF) devices have been studied in human and veterinary medicine. Placing the tPEMF loop (Assisi Loop; Zomedica) at the site of discomfort, this technology helps to reduce pain and swelling by increasing endogenous production of endothelial nitric oxide. In photo biomodulation, the penetration of laser energy depends on the wavelength of the device (multiple products are available), though is typically fairly shallow. This is indicated for pain management, control of inflammation, and tissue healing. Sound therapy or extracorporeal shockwave therapy involves the release of a sudden, high-powered shock wave resulting in tissue modulation at a focused depth of tissue. Newer devices (X-Trode; Zomedica) require less sedation than previous models, and excellent pain relief immediately posttreatment has been reported, lasting days to weeks.
Quality of life
For everything we can do in practice, education of the client and changes to the pet’s environments are essential. At home, comfort and mobility are critical to a pet’s quality of life and changes can help a caregiver’s workload as well.
Nonskid flooring or yoga mats can be placed on slick floors. Nail grips or booties can help with traction and foot placement. Raised food and water dishes can make mealtimes more comfortable, even using exercise balls to help support the pet as they eat. Comfortable, orthopedic bedding can be very beneficial, as can steps and ramps if they sleep in bed with the owners.
Ramps can also be used for negotiating some steps and getting in and out of vehicles. Especially with larger dogs, assistive devices such as harnesses and slings can be very beneficial to help them get up from a down or sitting position, and walking.
Conclusion
Although not just the “old dog disease” we usually consider OA to be, recognizing and managing all pets with acute or chronic joint pain can be an important part of your practice. In addition to therapies and disease management, the ideas for comfort and improving quality of life can also be used in practices to make these spaces more senior friendly.
Heidi Lobprise, DVM, DAVDC, is a veterinary dental specialist with Main Street Veterinary Hospital and Dental Clinic in Flower Mound, Texas, with an interest in senior pet care.