Emergency Evaluation of Effusions - Sample Handling, Cell Identification, Important Findings
An acute abdomen is defined as the acute onset of abdominal pain. Possible underlying etiologies are broad ranging, and include the gamut from trauma to infectious and neoplastic causes.
An acute abdomen is defined as the acute onset of abdominal pain. Possible underlying etiologies are broad ranging, and include the gamut from trauma to infectious and neoplastic causes. An effusion is defined as the escape of fluid into a part. Effusive processes can occur in essentially every tissue in the body. The ability to obtain this fluid for cytologic evaluation limits the types of samples that are amenable to examination. Synovial fluid, aqueous humor, cerebrospinal fluid and serous body cavity fluids are all routinely evaluated in veterinary medicine. Obtaining and rapidly assessing effusions are keys to the diagnosis, choice and institution of therapy, and the ultimate outcome of many cases.
Normal effusions are due to a combination of factors including Starlings forces, pressure differential across the visceral pleura that favors absorption, lymphatic drainage, mesothelial cell activity and the stoma between mesothelial cells. The different cavities can have a large, ongoing exchange of fluid and solute, yet a low, stable volume is maintained. Crudely, effusions form when there is an imbalance between formation and resorption
The power of the clincopathologic evaluation of effusions is undeniable. Using widely available tools and instruments, samples can be obtained with minimal risk to the patients, yet the diagnostic yield can be tremendous, depending on the specific disease entity present. The indication to obtain and evaluate fluid is often determined based on the history, physical examination, radiographic / ultrasonographic findings or other finding.
The proper handling of fluid can dramatically affect the diagnostic yield from samples otherwise properly obtained. If in doubt, contact your reference lab for details concerning submissions. EDTA containing tubes are ideal for cytologic analysis, as it provides the best morphology, with minimal distortion if smears are made relatively quickly. This tube can also be used for determination of the total nucleated cell count (TNCC) / white blood cell (WBC) count, total protein (TP) (assessed by refractometry) and packed cell volume (PCV). If cells are left in EDTA tubes, they will age naturally and artifactually become vacuolated. Likewise, if left in tube, in vitro phagocytosis (RBCs, bacteria, WBCs, etc.) will occur. EDTA is bacteriostatic and therefore not appropriate for culture. Tubes without additive (i.e. red topped tubes) can be utilized if any biochemical assays are to be performed on the sample. Although not ideal, they can be used for culture, mainly aerobic. Even clear samples can contain enough fibrin to compromise cytologic evaluation. Serum separator tubes (SST) should be avoided, as the gel can entrap cells and severely compromise cytologic evaluation. These tubes are likely ok for biochemical analysis. Culture tubes / Culturettes are often utilized based on cytologic findings. These should be utilized if cultures are to be performed. Individual labs may have specific media for specific tests (e.g. Mycobacterium sp., fungal isolation, virus isolation, anaerobic bacteria, etc.) and/or for transportation, especially if there will be a delay between sample acquisition and processing. If no better options are available, a sample can be submitted in the syringe for culture as long as it was obtained using sterile technique. The air should be expressed out of the syringe and securely capped. If possible, centrifuged sediment should also be submitted on media for culture. Heparin containing tubes can be used for biochemical assays, especially STAT samples



Unless otherwise noted, sample preparation should be done using fluid from the EDTA. Direct smears using the blood smear technique is an extremely simple, fast technique to visualize nucleated cells in an effusion that has moderately high to high TNCC (>10,000/μl). This is the preparation that should be consulted if there are concerns about true, in vivo changes to cells and/or structures in the background. A drop of the fluid is placed on one end of a clean, new slide. The spreader slide is backed up into the drop, which then spreads towards, but not to the sides. The spreader slide is then advanced off the slide in one firm, smooth motion, producing a bullet shaped smear:
The line technique is useful for making smears from samples with moderate nucleated cellularity. This technique is identical to the blood smear technique; however, the spreader slide is stopped short of the edge and lifted straight up, producing a line. No feathered edge is present; rather the nucleated cells are concentrated at the line formed by stopping the slide, which are then in a location on the slide where they can be evaluated.


Concentrated smears are used when the TNCC is <5,000 / μl. The smear is made by centrifuging a sample (1,000 – 1,500 rpm for 5 – 10 minutes OR 165 to 360G), pouring off the supernatant and re-suspending the remaining pellet with 0.5 ml of fluid. The smear is then made from the concentrated solution similar to making a blood smear. A buffy coat preparation is a useful technique that is used when there is heavy hemodilution or a relatively low TNCC. A portion of fluid is spun in a micro-hematocrit tube. The tube is then broken at the level of the buffy coat, which is then applied to a slide and streaked out as a blood smear. Cytocentrifuge preparations are very useful for samples with an extremely low TNCC, such as pure transudates. Albumen can be added to help preserve morphology. This technique requires a special centrifuge. A small amount (e.g. 0.5 ml) of sample is loaded into the funnel, which is clamped to the slide, sandwiching filter paper between the two. The sample is spun at 700–1,000 rpm for 10 minutes, Spinning the cells directly onto the slide, while the supernatant is wicked away by the filter paper. Affordable, home-made devices can also be made that utilize gravity to sediment the cells; however, they take too long in an emergency situation.
Several options are available for staining the smears; however, a majority of cytopathologists prefer one of the polychromatic Romanowsky stains. Diff-Quik or an equivalent is very easy to use, rapid, affordable and widely available. It offers good cellular and nuclear detail. Care must be taken to maintain the stains for consistent results. Wright's stain is occasionally used in higher volume settings. It provides excellent contrast and crisp colors for both the cytoplasm and nucleus. Gram stain can be useful for categorization of bacteria to aid in selecting initial antibiotic therapy; however, cellular features are poor. A control slide is an absolute must when using this stain.
The evaluation of an effusion starts with the gross examination. It is a valuable part of the overall assessment of a fluid sample. This process starts as the sample is being collected. A clean, lined note card may be useful in assessing color and turbidity of the straight sample. Normal fluid is pale yellow to straw colored. The color of a straight solution may be due to particulate matter such as: cells, fibrin, ingesta and clots; however, pigments such as hemoglobin, myoglobin, melanin and bilirubin can also cause a color change from normal. Changes in color of the supernatant after centrifugation implies that the color was due to something particulate. Examples of non-particulate material includes: hemoglobin, myoglobin, bilirubin and lipid.
Normal fluid is clear to slightly turbid or opalescent. Opacity of the straight fluid can be evaluated by looking at a lined note card or newsprint through the tube. Opacity could be due to particulate matter such as cells, protein clumps, necrotic debris or lipid. Anything that is removed via centrifugation is considered particulate. Examples include: cells, fibrin clumps, cellular debris and exogenous debris.
The odor of a fluid can also provide additional insight. Anaerobic infections tend to cause a foul odor; however, the lack of a foul odor does not rule out their presence. Samples from a uroabdomen can smell like ammonia, especially when warmed slightly.
Chemical analysis of fluids can help verify or better characterize the effusion based on the gross and microscopic findings. Total protein (TP) is one half of the criteria used to broadly classify effusions. It can be determined biochemically using the supernatant and a chemistry analyzer or can easily be estimated using a refractometer and the supernatant. A small sample in an EDTA tube will cause false elevation as will high concentrations of bilirubin or hemoglobin. Lipid will prevent accurate reading of the TP all together.
Other analytes The supernatant from either a clot tube or a heparin containing tube should be used, with the exception of glucose and lactate. Triglycerides, cholesterol, glucose, lactate, pH, creatinine, potassium, lactate dehydrogensase (LDH), amylase and lipase are examples of analytes that can be useful in better characterizing effusions.
The Total Nucleated Cell Count (TNCC) / White Blood Cell count (WBC) is the second main criteria used to broadly classify effusions. Cell counts can be artifactually low if EDTA tube is less than ¼ filled. The TNCC can be done manually with the Unopette (Becton Dickinson, Rutherford, NJ) system or it can be measured using an automated cell counter / CBC analyzer. Cell clumping (especially with excess fibrin present), cell fragmentation and debris can be misinterpreted as intact solitary cells using both systems. The Red Blood Cell count (RBC)
PCV can be easily performed using microhematocrit tubes or an RBC count can often be generated by automated counters. A PCV of the fluid greater than peripheral blood suggests aspiration of the spleen.
TP and TNCC are used in concert to classify effusions. The classifications are used to help focus on a set of differential diagnoses; however, they are not all inclusive and have ample overlap. Specific effusions (e.g. chylous, hemorrhagic, etc.) may be named as such, with or without other designations.
Pure transudate / Transudate is what is normally present within the cavity (if enough is present to obtain and analyze). It should be colorless to amber in color and clear in opacity. The TNCC is low, generally <1,000 – 1,500/μl. The cells present are usually a mixture of large mononuclear cells (mesothelial cells and macrophages) and small lymphocytes, with rare non-degenerate neutrophils also seen. The TP is low, <2.5 g/dl. The actually value is likely around 1.5 g/dl; however, 2.5 g/dl is the lowest reliable reading on many refractometers.
Differential diagnoses include hypoproteinemia (especially hypoalbuminemia <1.0 g/dl) of a variety of causes, leakage of lymph from lymphatics and acute uroperitoneum. A modified transudate is an effusion with increase in TP, without concomitant increase in TNCC OR vice-versa. Their color is variable; however, usually amber in color and clear in opacity. When elevated, the TP is usually 2.5 – 7.5 g/dl. Likewise, the TNCC is often slightly increased, 1,000 – 7,000μl. The proportions of cells present varies greatly, depending on the nature of the effusion. This class of effusions is generally non-specific in origin. Cytologic evaluation, as well as other tests is usually helpful in determining cause. Chylous, bilious, hemorrhagic and neoplastic effusions often fall under this category as do diseases associated with increased hydrostatic pressure (e.g. liver disease, right-sided or bi-ventricular heart failure, etc.). Effusions secondary to FIP can also fall under this category. Uroperitoneum can present as a modified transudate, once inflammation has contributed to the effusion. An exudate is an effusion that has an increased TP AND TNCC. TP is > 3.0 g/dl and the TNCC is >7,000/μl. Neutrophils frequently predominant and can be degenerate if an agent (e.g. bacteria, endotoxin, lipase, etc.) is present to kill them. Non-degenerate neutrophils and/or lack of visualization of an agent do not rule out its presence. Other causes include bile peritonitis, chronic uroperitoneum, acute pancreatitis, recent celiotomy and necrosis.


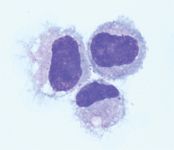
Non-activated macrophages, 60x, Modified Wright's
The microscopic examination is where a bulk of the information garnered from an effusion is obtained. Red blood cells are generally ignored other than to determine he presence of in vivo hemorrhage or inflammation. Caution is encouraged when interpreting RBC morphology; however, hemoparasites can rarely be detected. If there is suspicion of a specific poikilocyte such as an acanthocyte, venipuncture and blood smear examination should be pursued. Mesothelial cells are simple squamous cells that form a sheet lining the serosal cavities and are invariably present in effusions. More tend to become more plentiful with more fluid present. They can be seen as singlets as well as in small to large cohesive clusters. These cells are generally grouped with macrophages into a group referred to as "Large mononuclear cells". When non-reactive, these cells are small to medium in size. They generally contain a single, centrally place nucleus set in a moderate amount of lavender cytoplasm. The nuclei exhibit a finely reticular chromatin pattern and infrequently contain a few small nucleoli. They can have a bright pink, ruffled cell margin called the corona, which is an artifact of slow drying and is of no diagnostic significance. Mesothelial cells easily become reactive due to many things, primarily inflammation. When reactive, these cells become markedly atypical, and will display numerous strong criteria of malignancy. The cytoplasm will turn dark blue to dark purple and can vacuolate. Polykaryosis is common as are marked anisocytosis and anisokaryosis (between cells as well as within multinucleated cells). The nuclei will exhibit a coarse chromatin pattern and frequently will contain one to several, variably sized, markedly pleomorphic, prominent nucleoli. Reactive mesothelium will become phagocytic and thus cells and debris can be seen within them. Differentiation between reactive / hyperplastic mesothelial cells and cells associated with malignant neoplasia (i.e. mesothelioma, carcinomatosis, etc.) presents a major diagnostic challenge that even the most seasoned cytopathologist cannot unravel. Non-activated macrophages are small to large in size and generally contain a single round to ovoid nucleus set in a moderate amount of blue, smooth to lightly vacuolated cytoplasm. Occasional bi-nucleate and tri-nucleate cells can be found. The nuclei exhibit a lacy, fine chromatin pattern. These cells are nearly identical in morphology to non-reactive mesothelial cells.
When activated these cells have more abundant, more basophilic cytoplasm than their non-reactive counterparts. They also have ruffled cytoplasmic margins, prominent cytoplasmic vacuoles and/or inclusions. Lymphocytes are occasionally seen in effusions. Their percentage may increase in response to chronic inflammation, parasitism and in chylous effusions. They can re-circulate into peripheral blood. They are usually 1.5 to 2 times the diameter of an RBC and have a single round to slightly indented nucleus with a condensed chromatin pattern. These cells possess light to sky blue colored cytoplasm. They consistently exhibit a high N:C ratio. Reactive lymphocytes have more cytoplasm than their non-reactive counterparts, which is dark blue in color and may have a small, perinuclear clearing. Neutrophils are frequently present in samples as a true in vivo entity as well as secondary to blood contamination. If present solely due to contamination, their morphology should be identical to that in the peripheral blood and should be present in the same proportion compared to RBCs (roughly 400:1). Once it is determined that they are not present due to contamination, they are considered pathologic, as neutrophils are not tissue residents like macrophages and eosinophils. Every time neutrophils are assessed, their level of degeneration must be evaluated. This must be done in an intact cell. Assessment of degeneration should be made in a monolayer portion of the smear to avoid the changes associated with mechanical stress. Determining degenerate changes is of utmost importance, as their state can greatly affect the decision to manage medically vs. surgically. Non-degenerate neutrophils look essentially just like they did in circulation. Toxic changes may be observed, which are generally cytoplasmic in nature (e.g. Döhle bodies, blue foamy cytoplasm and toxic granulation). These changes are not assessed in cytologic preparations per se, as their significance is reserved for hematologic evaluation as they occurred during granulopoiesis. Non-degenerate neutrophils suggest an environment that is not particularly harsh; however, occasionally bacteria with weak toxins (e.g. Actinomyces spp.) can be present with non-degenerate neutrophils. Degenerate changes indicate that a cell has been killed or sustained lethal injuries and therefore cannot voluntarily go into apoptosis. The damage is due to local factors such as bacterial toxins, bile, mediators associated with pancreatitis, etc. These changes are nuclear and result from changes in permeability of the nuclear membrane, allowing water into the nucleus, which ultimately leads to single cell necrosis. If doubts are present as to the amount of degenerate changes present in a "processed" smear, refer to freshly made, direct smears. Karyolysis is swelling of the nucleus, with loosening of chromatin pattern as well as a less purple to magenta colored chromatin, rather than condensed and dark purple of a non-degenerate neutrophil (Romanowsky stains). Nuclear margins also tend to become fuzzy and indistinct. This proceeds to hyalinization of the nucleus and eventual dissolution. These changes occur in an intact cell.
Karyorrhexis is when the nucleus fragments into numerous small dark, hyperchromic spheres. Neutrophil tissue life is measured in hours and they do not re-enter the blood stream. Once their life is spent, they will undergo apoptosis and eventually be phagocytized by macrophages (i.e. leukocytophagia, leukophagia, cytophagia).
Hypersegmentation is when the neutrophil nuclei have greater than five lobes and is often accompanied by thinning of the intra-nuclear bridges. This change is a precursor to pyknosis. Pyknosis occurs when the intranuclear bridges break down and the lobes condense into one a few hyperchromic structures. The cells themselves will often condense and their cytoplasm will stain more intensely pink than their viable counterparts. Eosinophils, mast cells and neoplastic cells can all be seen in effusions, depending on the nature of the effusion. Artifacts such as glove power (a crystalline structure) and ultrasound gel (bright magenta amorphous material) as well as stain precipitate must be identified and ignored.
Being able to rapidly obtain, process and evaluate effusions can provide a powerful tool that can be used to diagnose numerous processes and allow the clinician to make sound clinical decisions. Details concerning specific effusions will be discussed including: septic, bilious, chylous and hemorrhagic effusions.
References
Aumann M, Worth LT, Drobatz KJ. Uroperitoneum in Cats: 26 Cases (1986 - 1995). Journal of the American Animal Hospital Association. 34: 315-324. 1998.
Baker R, Lumsden JH. Pleural and Peritoneal Fluids in Color Atlas of Cytology of the Dog and Cat. Raskin RE and Meyer DJ Eds. Mosby, St. Louis. 2000.
Beal MW. Approach to the Acute Abdomen. Veterinary Clinics of North America (Small Animal).35(2): 375-396. 2005.
Connally HE. Cytology and Fluid Analysis of the Acute Abdomen. Clinical Techniques in Small Animal Practice. 18(1): 39-44. 2003.
Cowell RL, Tyler RD, Meinkoth JH. Abdominal and Thoracic Fluid in Diagnostic Cytology and Hematology of the Dog and Cat 2nd Ed. Cowell RL, Tyler RD, Meinkoth JH Eds. Mosby, St. Louis. 1999.
Crowe DT, Bjorling DE. Peritoneum and Peritoneal Cavity in Textbook of Small Animal Surgery 2nd Ed. Slatter D ed. W.B. Saunders. Philadelphia. 1993.
DeHeer HL, Parry BW, Grindem CB. Peritoneal Fluid in Diagnostic Cytology and Hematology of the Horse 2nd Ed. Cowell RL, Tyler RD Eds. Mosby, St. Louis. 2002.
Grindem CB, Fairley NM, Uhlinger CA, Crane SA. Peritoneal Fluid Values from Healthy Foals. Equine Veterinary Journal. 22(5): 359-361. 1990.
Hartmann K, Binder C, Hirschberger J, et al. Comparison of Different Tests to Diagnose Feline Infectious Peritonitis. Journal of Veterinary Internal Medicine. 17: 781-790. 2003.
Hirschberger J, DeNicola DB, Hermanns W, Kraft W. Sensitivity and Specificity of Cytologic Evaluation in the Diagnosis of Neoplasia in Body Fluids from Dogs and Cats. Veterinary Clinical Pathology. 28(4): 142-146. 1999.
Kjeldsberg C., Knight J. eds. Body Fluids: Laboratory Examination of Amniotic, Cerebrospinal, Seminal, Serous & Synovial Fluids 3rd Ed. ASCP Press, Chicago. 1993.
Kruth SA. Abdominal Distention, Ascites and Peritonitis in Textbook of Veterinary Internal Medicine 6th Ed. Ettinger SJ, Feldman EC eds. Elsevier Saunders, St. Louis. 2005.
Macintire DK. The Acute Abdomen Differential Diagnosis and Management. Seminars in Veterinary Medicine and Surgery (Small Animals) 3(4): 302-310. 1988.
Mazaferro EM. Triage and Approach to the Acute Abdomen. Clinical Techniques in Small Animal Practice. 18(1): 1-6. 2003.
Orton EC. Pleura and Pleural Space in Textbook of Small Animal Surgery 2nd Ed. Slatter D ed. W.B. Saunders. Philadelphia. 1993.
Rudloff E. Abdominocentesis and Diagnostic Peritoneal Lavage in Textbook of Veterinary Internal Medicine 6th Ed. Ettinger SJ, Feldman EC eds. Elsevier Saunders, St. Louis. 2005.
Shelly, SM. Body Cavity Fluids in Atlas of Canine and Feline Cytology. Raskin RE, Meyer DJ Eds. W.B Saunders, Philadelphia. 2001.
Tyler RD, Cowell RL. Evaluation of Pleural and Peritoneal Effusions. Veterinary Clinics of North America: Small Animal Practice. 19(4): 743-768. 1989
Van Hoogmoed L, Rodger LD, Spier SJ, et al. Evaluation of Peritoneal Fluid pH, Glucose Concentration, and Lactate Dehydrogenase Activity for Detection of Septic Peritonitis in Horses. Journal of the American Veterinary Medical Association. 214(7): 1032-1036. 1999.
Van Hoogmoed L, Snyder JR, Christopher M, Vatistas N. Peritoneal Fluid Analysis in Peripartum Mares. Journal of the American Veterinary Medical Association. 209(7) 1280-1282. 1996.
Walters JW. Abdominal Paracentesis and Diagnostic Peritoneal Lavage. Clinical Techniques in Small Animal Practice. 18(1): 32-38. 2003
Walters PC. Approach to the Acute Abdomen. Clinical Techniques in Small Animal Practice. 18(1): 63-69. 2003
Zocchi L. Physiology and Pathophysiology of Pleural Fluid Turnover. European Respiratory Journal. 20: 1545-1558. 2002.













Podcast CE: A Surgeon’s Perspective on Current Trends for the Management of Osteoarthritis, Part 1
May 17th 2024David L. Dycus, DVM, MS, CCRP, DACVS joins Adam Christman, DVM, MBA, to discuss a proactive approach to the diagnosis of osteoarthritis and the best tools for general practice.
Listen



