Feeding tubes in small animal practice (Proceedings)
Nutritional support is required for anorexic patients, debilitated patients, patients in a high catabolic stage (peritonitis, sepsis, burns), or stressed patients (surgical patient).
Nutritional support is required for anorexic patients, debilitated patients, patients in a high catabolic stage (peritonitis, sepsis, burns), or stressed patients (surgical patient). Nutritional support allows a faster soft tissue healing, a better immune system response and a faster recovery from the patient. Nutritional support can be performed with food intake stimulation, force feeding, and feeding tubes. Vitamin B, valium (0.2 mg/kg IV) and ciproheptadine (2 mg/cat 2 to 3 times a day) have been used to stimulate food intake in dogs and cats with variable results. Force feeding with a syringe or tube is possible for one day or two. Force feeding places lot of stress on the animal and may induce aspiration pneumonia. Feeding tube placed either surgically or under endoscopy is the most efficient technique to provide nutritional support to a patient. Feeding tubes can be easily placed at the end of an abdominal surgery and may avoid lot of complications and troubles after surgery. Gastrostomy and jejunostomy tubes are the 2 most commonly used feeding tube in small animal. Esophagostomy tube and gastrojejunostomy tube are the feeding tubes used most commonly.
Nasogastric Tube
A nasogastric tube can be placed in dogs and cats if feedings need to be continued for more than 2 days. It is a good technique for the nutritional support of young animals. It does not require general anesthesia for its placement. A topical anesthetic (bupivacaine: 2 to 5 dropes) is placed into the nostril. Before placing the tube, the distance from the nares to the stomach needs to be measured. The stomach is located at the level of the last rib. A 3.5 French tube is recommended for puppies and kitten, while a 5.0 Fr tube can be used for adult cat and dogs less than 8 kg. With the animal's head held in a normal static position the tube is introduced in the nose in a caudo-medial direction ventral to the alar fold. Pushing the nose upward helps moving the tube downward in the ventral meatus. A stylet or guide wire might be useful to guide the tube in the correct direction. The tube progress through the larynx into the esophagus and the stomach. If the animal is coughing, the tube is more likely going into the trachea. A bolus of sterile saline ca be injected in the tube. If the animal coughs more likely the tube is in the trachea. If there is any doubts on the placement of the tube radiographs should be taken to confirm the placement of the tube in the stomach and not the trachea. Palpation of the trachea and the tube in the esophagus is a good indication for correct placement of the nasogastric tube. Since the tubes are small in diameter a liquid diet (Clinicare) is recommended. The tube needs to be flushed between feeding to prevent the tube from plugging.
Esophagostomy Tube
Several techniques have been described for placement of an esophagostomy tube placement in dogs and cats. The animal needs to be under general anesthesia. The entire left cervical region from the ventral to dorsal midline need to be clipped and prepared for surgery.
The left side of the cervical region is draped and a percutaneous feeding tube applicator (ELD Gastrostomy tube applicator) is inserted through the mouth in the proximal cervical esophagus. The tip of the ELD device is turned outward and the cervical tissue are tented up. A small skin incision is made just large enough to accommodate the feeding tube. The incision is made deeper to the esophagus and the sharp needle in the ELD is advanced to puncture through the esophagus. A feeding tube is attached to the needle. The needle is retrieved in the ELD device. The ELD device is retrieved through the mouth with the feeding attached. Now the feeding tube is going through the skin of the left cervical area, the esophagus, and exiting in the mouth. The tip of the tube is then redirected into the pharynx and the esophagus. The tube needs to be manipulated gently to prevent perforation of the distal esophagus. The tube is then secured with a Chinese finger trap suture. A light bandage is applied to protect the tube. The tip of the tube should be in the esophagus. It is then necessary to measure the length of the tube that could be placed in the esophagus without entering the lower esophageal sphincter. The lower esophageal sphincter is located at the level of the xyphoid. A large red rubber feeding tube can be placed with this technique. For a cat a 12 to 14 Fr tube can be placed and for a 30 kg dog a 20 Fr tube be used. It is recommended to increase the diameter of the hole at the tip of the tube to prevent obstruction of the tube with food.
An alternative technique is to use a large Carmalt or curve forceps for the placement of the tube instead of the ELD device. Forceps have a tendency to create a hole too large in the esophagus, which may result in leakage of saliva and food around the tube. It will induce a severe cellulitis, and abscess formation.
Blenderized food can than be used for the nutritional support of the patient. The animal is usually fed 4 times a day. The tube needs to be flushed after each feeding with copious amount of water. Tubes entering the stomach will induce vomiting. Some dogs or cats have been vomiting their tube.
Gastrostomy Tube
Gastrostomy tube are more commonly placed during abdominal exploration. However, they can be placed with a limited flank approach or percutenously with an endoscope.


Surgical Technique During Abdominal Exploration
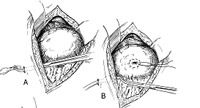
The greater curvature of the body of the stomach is identified. The greater curvature of the body of the stomach is manipulated to identify the are with e least amount of tension after placement against the left abdominal wall behind the last rib. A purse-string suture with 3-0 monofilament absorbable suture is placed in the gastric fundus in the identified area (Figure 1 B).
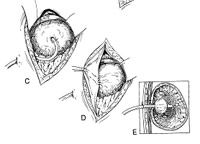
A Foley catheter (18 to 20 French) is inserted first through the left abdominal wall just behind the last rib (Figure 1 A). A stab incision is made in the middle of the purse-string suture and the tip of the Foley introduced in the stomach (Figure 2 C). The balloon of the Foley catheter is inflated with appropriate amount of saline and the purse-string suture tied. Four gastropexy sutures (3-0 monofilament absorbable material) are placed between the stomach wall and the abdominal wall (Figure 2 D-E). The sutures are evenly distributed around the Foley catheter. A Chinese finger tap suture is placed around the Foley catheter on the skin.


Flank Approach
After surgical preparation of the left flank, a rigid stomach tube is inserted through the mouth into the stomach. The stomach tube is rotated to tent up the skin of the left flank. With the tube maintained in place a skin incision is performed over the tube. Blunt dissection of the abdominal wall is performed over the tube. When the peritoneum is opened, the stomach wall is identified on the top of the tube. The stomach wall is then pexied to the abdominal wall with four mattress sutures. The stomach can then be removed. A purse-string is placed in the stomach wall and a Foley catheter is introduced after puncture with an #11 blade in the middle of the purse-string. The purse-string is tight and the skin closed. The Foley catheter can be tunneled under the skin before it penetrates in the stomach.
Percutaneous endoscopic gastrostomy tube placement
Percutaneous endoscopic gastrostomy (PEG) tubes are inserted with the aid of general anesthesia. The animal is placed in right lateral recumbency and the flank area behind the last rib is surgically prepared. The endoscope is introduced in the stomach through the mouth. The stomach is insufflated with carbon dioxide. The stomach wall is then getting in contact with the abdominal wall. The lighted tip of the endoscope is turned to visualize the wall of the body of the stomach. A large needle is inserted into the stomach under the control of the endoscope. A nylon suture is inserted in the needle and grabbed in the stomach with a grasper inserted through the endoscope. The suture is pulled through the mouth while the endoscope is withdrawn. A mushroom tip catheter is then attached to the nylon suture coming out through the mouth. The lubricated catheter is pulled into the stomach by the suture exiting the body wall. Resistance will be encountered when the tip of the catheter hit the stomach/body wall. Firm traction is applied o the suture and counter-traction is applied to body wall to be able to pull the catheter through. A rubber flinge is fitted down the tube to prevent slippage of the tube. The flinge is glued to the catheter.
The tube can be removed by applying firm traction of the tube that will collapse the mushroom. In large breed dog the mushroom can be cut and pass through the feces.
The gastrostomy tube is removed by cutting the Chinese finger trap, deflating the balloon and pulling the catheter. Very often, the balloon is ruptured after 2 weeks because of the acid content of the stomach. If the tube needs to be maintained for more than 2 weeks a mushroom tip catheter is preferred to a Foley catheter. The fistula between the stomach and the skin is going to close quickly. Usually there is no leakage of stomach content through the fistula.
Feeding is started 24 hours after placement of the gastrostomy tube. Leaks of food can occur around the tube if the feeding is started to early. The correct amount of gruel for the patient is administered through the catheter. The catheter needs to be flushed every 4 hours to prevent its obstruction. The tube needs to stay in place for at least 7 days before its removal to allow appropriate sealing of the pexy. The gastrostomy tube can be kept for several weeks. It is recommended to start feeding with 1/4 maintenance and to increase the caloric intake by 1/4 every day. If animal shows abdominal discomfort, vomiting or diarrhea the caloric intake is decreased by a 1/4. The amount of food required daily is divided in four feedings.
Jejunostomy Tube
A jejunostomy tube is placed when bypass of the upper part of the gastrointestinal is required. A loop of jejunum is selected distal to the part of the intestine that needs to be bypassed. A purse-string of 3-0 monofilament absorbable suture is placed on the antimesenteric border of the jejunum. The jejunostomy tube (3 to 5 French) is first inserted through the abdominal wall. A stab incision is made in the middle of the purse-string and the jejunostomy tube is introduced in the jejunum 20 cm aborally. The purse-string is tied. Then, four jejunopexy sutures are placed evenly around the jejunostomy tube between the abdominal wall and the jejunum.
Feeding can be started immediately after placement of the jejunostomy tube. A liquid diet is administered continuously through a feeding pump. The catheter needs to be flushed every 4 hours to prevent its obstruction. It is recommended to start feeding with 1/4 maintenance and to increase the caloric intake by 1/4 every day. If animal shows abdominal discomfort, vomiting or diarrhea the caloric intake is decreased by a 1/4. The tube needs to stay in place for at least 4 days before its removal to allow appropriate sealing of the pexy. Usually, the jejunostomy tube is for short-term usage because a pump is required to deliver the diet. Jejunostomy tube is advantageous for patients requiring multiple anesthesias (open abdominal drainage) or being profusely vomiting before surgery.
Gastro-Jejunostomy Tube
It is very common to place a gastrostomy and a jejunostomy tube at the time of surgery. The jejunostomy tube is for the short-term support of the vomiting patient and the gastrostomy tube for the long-term support of a severely debilitated patient. The gastrostomy is placed first as described earlier during an abdominal exploration. Then a jejunostomy tube is fed in the lumen of the gastrostomy tube into the duodenum and the proximal jejunum. The gastrostomy tube has to be of a large diameter (22 to 24 Gauge) to allow passage of the jejunostomy tube. The gastrostomy tube can then be used to aspirate stomach content to prevent vomiting and the jejunostomy tube can be used for feeding of the patient. When the animal is not vomiting, the feeding can be performed through the gastrostomy tube. The jejunostomy tube can then be removed. The advantage of this technique is that only one opening is required for the placement of the two feeding tubes. Gastro-jejunostomy kits are available. Each tube is managed as each tube placed separately.
















