Maxillary swelling in a 2-year-old cat: What's your diagnosis?
Discover why this feline is missing a canine.
A 2-year-old neutered male domestic longhaired cat is presented for evaluation of a maxillary mass protruding from the space normally occupied by the right maxillary canine, tooth 104 (Photo 1). The swelling is hard throughout its circumference but has a fluctuant portion on its ventral aspect. The patient's history reveals no apparent discomfort, and a pain response is not elicited on palpation. The owners cannot recall whether a tooth was present before the appearance of the swelling. Based on this information, what is your No. 1 rule-out for this swelling?



Photo 1: This 2-year-old cat has a mandibular mass protruding into the vestibule from the space normally occupied by the right maxillary canine.
Differentials and definitive diagnosis
Neoplasia, particularly odontogenic tumors, must be considered. Infection is possible but unlikely because of the character of the mass and the lack of pain on palpation. The most likely cause is a dentigerous cyst associated with the right maxillary canine tooth. Although definitive diagnosis can only be made with histopathology, dental radiography is extremely valuable in determining the cause in these cases. Photo 2 shows the tooth displaced caudally and toward the midline within the relatively lucent right maxilla.
During normal adult tooth development, the inner and outer enamel epithelia are responsible for producing the enamel of the mature tooth. Once the enamel is formed, these tissues fuse to become the reduced enamel epithelium. Picture this as a tight sac around the enamel. As the tooth erupts, this tissue becomes the junctional epithelium, which is the tissue present at the base of a normal pocket (sulcus). When you place a periodontal probe into a normal sulcus, the probe rests on this tissue. Dentigerous cysts often form when the tooth fails to erupt and this epithelial tissue remains within bone. Osmotic gradients cause this epithelial sac to take on fluid. Unfortunately, these cysts can expand to the point of causing severe destruction of bone, adjacent teeth and surrounding tissue.

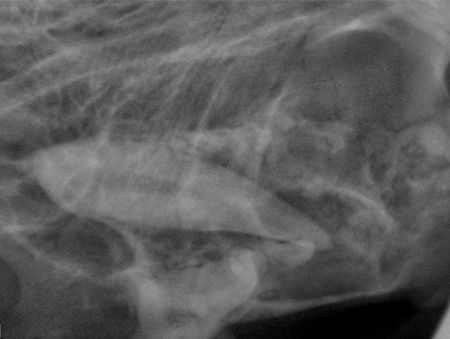
Photo 2: The canine tooth is displaced caudally and toward the midline within the relatively lucent right maxilla.
Treatment
The surgical approach to resolution in this case involved a mucogingival flap to expose the underlying bone (Photo 3). Clear fluid exuded from the ventral aspect of the initial incision. The exuberant bone was removed with a dental bur, and the defect was enlarged to aid in visualization.



Photo 3: A mucogingival flap has been created to expose the underlying bone.Cyst material was then removed in pieces with the aid of a periosteal elevator, thumb forceps and a hemostat (Photo 4). In this patient, the progressive growth of the cyst expanded the vestibular bone and overlying gingiva to produce the mass effect. The lateral wall of the nasal cavity was compromised. The palatal wall of the infraorbital canal wall was obliterated, exposing the infraorbital neurovascular bundle.



Photo 4: Some of the cyst epithelium has been curetted from the bone dorsal to the defect and is seen here at the opening of the defect prior to removal.
The tooth itself was forced caudally and toward the palatal midline residing within the maxillary sinus at its caudal extent. The suction wand can be seen radiographically at the caudal-most point of cyst expansion (Photo 5). The tip lies within suborbital bone.
Treatment for dentigerous cysts involves removal of the cyst lining and the tooth while avoiding vital structures within the bone. Any teeth in which the apex has been compromised should be extracted. Teeth in which the apex is preserved but cementum is destroyed may be salvageable but must be followed radiographically to ensure viability. In this case, suction, surgical magnification, and meticulous cyst removal was vital around the infraorbital vasculature and nerves.


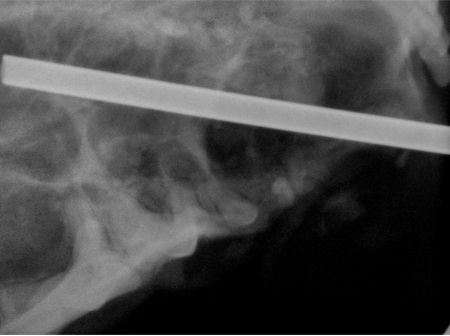
Photo 5: The tip of the suction wand can be seen here at the caudal extent of the cyst's expansion.Once cyst excision and extraction were complete, a postoperative radiograph confirmed complete removal of the tooth, and the mucoperiosteal flap was trimmed and sutured in a simple interrupted pattern with 4-0 absorbable monofilament suture material (Photo 6).



Photo 6: The flap is trimmed and closed with simple interrupted sutures.
Overview
Quite unlike this patient with an obvious mass that led to detection, most dentigerous cysts do not produce clinical signs in their early stages. Dogs are particularly predisposed to dentigerous cysts, most commonly associated with an unerupted mandibular first premolar. Brachycephalic breeds appear to be overrepresented (Photo 7). Expansion is generally within the bone and not in the surrounding gingiva.
Any patient that lacks a full dentition past expected normal eruption requires dental radiography to rule out unerupted teeth. Early intervention with extraction of these teeth in young patients is paramount in prevention. Treatment depends on the oral surgical skills of the practitioner, but most cases should be referred to a dental specialist. Make a habit of counting teeth in all patients, and you will find that this problem is more common than you thought.



Photo 7: An unerupted first premolar has resulted in a cyst in this 3-year-old brachycephalic dog.
Newsletter
From exam room tips to practice management insights, get trusted veterinary news delivered straight to your inbox—subscribe to dvm360.














