Oral surgery solutions: A look at difficult cases in dentistry
Periodontal disease is common in veterinary medicine and often requires surgical intervention. But some cases are more challenging than others-and knowing when to refer is key for good outcomes.
Next >
Most of the dentistry services we provide our patients in general veterinary practice involve the diagnosis and treatment of periodontal disease. Extractions make up a large portion of the oral surgery performed for this condition. At times we are faced with the unusual or difficult case that, depending upon the skill level and experience of the surgeon, may require referral to a board-certified specialist. This is the first in a series of articles examining these challenging oral surgical cases.
Extraction gone bad
An 8-year-old neutered male Cavalier King Charles spaniel was presented for oral pain following extraction of a fractured left mandibular fourth premolar (308). Partial anorexia and pawing at the left side of the face were noted by the owner immediately following the procedure and persisted for three weeks up to the time of referral. The referring veterinarian confirmed that the mesial root fractured upon attempted extraction and the apical fragment was forced into the mandibular canal in an attempt to retrieve it with a luxator.



Figure 1: View of the healed extraction site of the left mandibular fourth premolar in a Cavalier King Charles spaniel. (All photos courtesy of Dr. Brett Beckman.)
Visual examination of the left mandible indicated normal mucosa at the extraction site (Figure 1). Radiographs confirmed a fractured root tip in the mandibular canal ventral to the alveolus of the mesial root of tooth 308 (Figure 2, white arrow). A diffuse radiodensity was also evident just distal to the root tip (Figure 2, black arrow). The assumption was that this radiodensity consisted of fragments of alveolar bone.


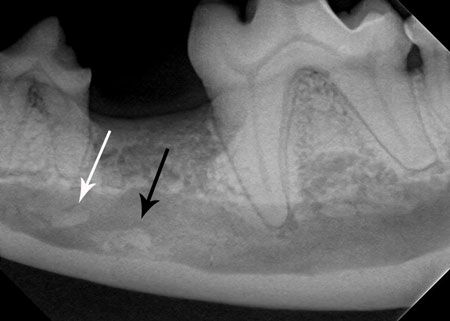
Figure 2: Radiograph of the left mandible demonstrating an apical root segment (black arrow) and bone fragments (white arrow).
Due to the location of the root tip and presumed bone fragments, a lateral approach was considered the most likely procedure to result in visualization and retrieval. In comparison, a dorsal approach provides limited access and visualization due to the two adjacent teeth and the distance from the bone to the fragments. Attempt at retrieval with a dorsal approach can result in mesial or distal migration of the fragments, which would then require a lateral approach.
A caudal mandibular nerve block was administered using 0.5 ml of 0.5% bupivicaine five minutes prior to the procedure. An incision was made in the alveolar mucosa 3 to 4 millimeters apical to the mucogingival junction at the level of the mandibular canal. A round bur was utilized to create a small bone defect for placement of a periodontal probe. A radiograph was taken with the probe tip within the defect to confirm the relative position of the proposed ostectomy (Figure 3).


Figure 3: A radiograph was taken with the probe tip within the defect to confirm the relative position of the proposed ostectomy.
A No. 4 round bur was used to remove bone in an elliptical pattern to the point that the mandibular canal could be visualized through the thin remaining bone for the entire length of the ostectomy site. A fine No. 4 round diamond bur was used to complete the ostectomy, carefully avoiding traumatic entry into the canal to protect the inferior alveolar neurovascular structures (Figure 4).

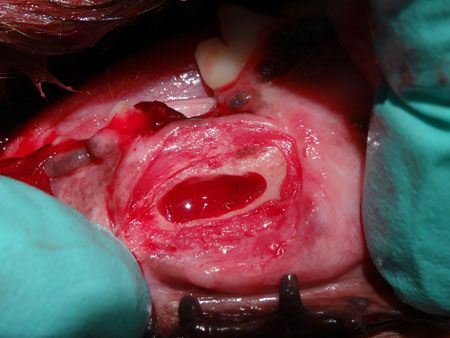
Figure 4: View of the exposure in the lateral aspect of the mandibular body created to remove the root tip and bone fragments.
The root tip and several small fragments of alveolar bone were removed from the ventral and lingual aspect of the mandibular canal by carefully retracting the neurovascular structures using a feline periosteal elevator. Extension of mesial and distal observation revealed complete removal of all root and bone fragments. A radiograph was taken to confirm the absence of all fragmented material (Figure 5). A blood clot was left and the defect was closed in two layers. The patient demonstrated no additional signs of pain following the surgical procedure.

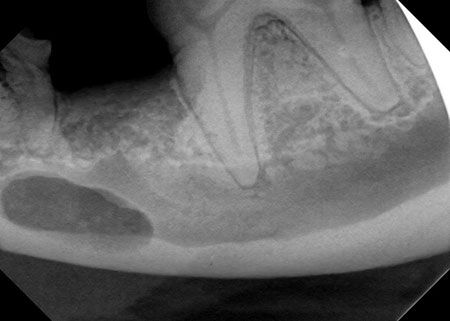
Figure 5: Postoperative view of the site confirming complete removal of bone and tooth root.
Congenital soft palate defect in a cat
An 11-month-old cat presented for chronic nasal discharge (Figure 6) and a considerably large congenital soft palatal cleft (Figure 7). The bilateral cleft extended from the midline to just medial to the palatoglossal folds. Clefts of this type are often associated with additional signs of coughing, gagging and sneezing. Aspiration pneumonia is a common complication.



Figure 6: An 11-month-old domestic short-haired cat with chronic bilateral nasal discharge.


Figure 7: A bilateral congenital soft palatal cleft.
Repair of congenital clefts in young animals should ideally be delayed until the patient is at minimum 8 weeks of age. Many of these patients demonstrate mild to moderate clinical signs that can be managed until the ideal time of 16 weeks of age. Surgery at this time provides more tissue and an ideal blood supply for an excellent prognosis for complete closure.
The surgical approach requires patient positioning in dorsal recumbency. Mucus is often present (Figure 8) and evident upon positioning and should be removed with cotton tipped applicators. A thin muscular layer separates the oral and nasal palatal mucosa. A small stab incision is created at the rostral aspect on each side of the defect. Scissors are used to extend the separation of the oral and nasal mucosal layers to the caudal extent of the defect. Further lateral dissection allows for mobility of each layer enabling tension-free primary closure (Figure 9). The nasal layer is closed with simple interrupted sutures using 5-0 monocryl. The same suture material and pattern is then used to close the oral mucosa (Figure 10).


Figure 8: Mucus is present in the nasopharynx and is removed prior to surgery.

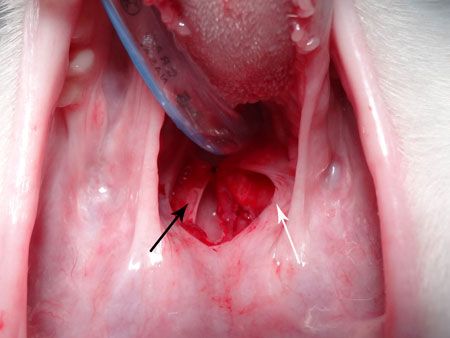
Figure 9: The nasal (black arrow) and oral (white arrow) mucosa following dissection to separate the layers prior to closure.

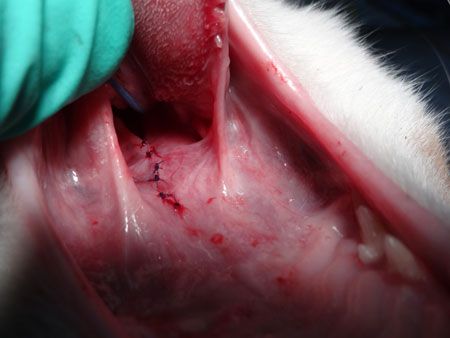
Figure 10: Simple interrupted sutures are used to close the nasal and the oral mucosa.
The primary concern with this defect was closure without tension due to the large size of the defect. Careful dissection and delicate tissue manipulation is required to minimize trauma and maintain blood supply to ensure full closure. This patient experienced a complete recovery with elimination of clinical signs (Figure 11).


Figure 11: Four weeks postoperatively shows complete closure of the defect.














