Review of the blood smear cell identification, morphology, and parasites of the three main cell lines (Proceedings)
Evaluation of a properly prepared blood smear by the trained human eye is an absolutely necessary compliment to machine evaluation of peripheral blood in all species.
Evaluation of a properly prepared blood smear by the trained human eye is an absolutely necessary compliment to machine evaluation of peripheral blood in all species. From the first generation table top complete blood count (CBC) analyzers to machines that fill half a room and cost hundreds of thousands of dollars, a machine generated CBC has numerous limitations. These limitations produce holes in the data that could be derived from the peripheral blood that, if left unfilled, can lead to misdiagnosis (including non-diagnosis), inappropriate therapy, or other preventable errors that result in inadequate patient care. This lecture is meant to be a guideline that can be used to navigate your way through a blood smear and get all of the important information on a routine basis. The role of the technician in this process is indispensable, as they often provide the initial, rapid evaluation of samples that they obtained and prepared. Initial treatments and choice of advanced diagnostics can hinge on the information provided. In depth pathophysiology, information treatment information, etc. can be found in any number of excellent sources listed in the references at the end.
The first step to evaluation of the peripheral blood is to obtain a sample. Ethylenediaminetetraacetic acid (EDTA) is the anticoagulant of choice for white blood cell (WBC) morphology. Citrate can be used if platelet or white blood cell (WBC) clumping occurs. If possible collection directly into a vacuum tube is preferred, using the largest needle size possible to minimize hemolysis. Use the largest free-flowing vein possible to minimize hemolysis. Fill tube to full, as dictated by the amount of vacuum in the tubes.
Once a sample is obtained, several smears should be made from the fresh sample. Preparing a diagnostic blood smear is something that takes practice, yet over time will become almost a reflex. A properly made blood smear is indispensable to a complete examination. Place a new clean slide on a firm, level surface. Using a sample that is grossly free from clots, place 2-3mm drop of well-mixed blood near one end of the slide or label. Keeping the spreader slide at a 30º angle, it is backed into the drop of blood. Allow the drop to spread towards, but not TO, the sides of the slide. In one smooth, firm motion, move the spreader slide directly toward the end of the slide and off the edge. The smear produced should be bullet shaped and not reach the end of the slide
Figure 1- The spreader slide is backed into the drop of blood until the two touch. Capillary action will spread the drop towards the edge of the slide.



Figure 1
Figure 2- Before the drop reaches the edge of the slide, the spreader slide is pushed forward in a single smooth motion, streaking out the drop of blood into a bullet shaped smear that does not reach the end of the slide.


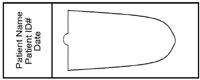
Figure 2
Inappropriate smears include those with chatter in them, smears that reach the edge(s) or end of the, smears that abruptly end, smears that curve off to one side.
Microscopic evaluation begins with a low power (10x or 20x) scan (Figure 4). This initial scan allows rapid evaluation of the whole smear that is an important part of the overall evaluation, even though this scan should take no more than 30 seconds Figure 3- One pattern of low power scan that encompasses all major components of the smear


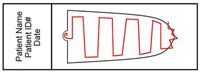
Figure 3
This initial scan allows one to get an overall estimate of white blood cell (WBC) mass. This scan is also used to observed important leukocytes or other nucleated cells that may be present low numbers that may be missed on a 100 or even 200 cell differential. Another important thing that this scan provides is a microscopic assessment of WBC clumps. The low magnification scanning is ideal for identifying specific arrangements that may not be so obvious when viewed at high magnification such as agglutination and rouleaux. Platelet clumps can be easily found with a low power scan, thus invalidating any absolute number produced by a machine or by estimate on the smear.
Microfilaria (e.g. Dirofilaria immitis, Dipetalanema sp.) can also easily be picked up on a low power scan.
The high power evaluation (50x - 60x) is ideal for doing WBC differential counts in the monolayer of the smear. The monolayer is defined as the area of the smear where half of the erythrocytes touch. This magnification is a perfect blend of detail and area covered. Examination at100x is necessary to observe fine hemoparasites, chromatin patterns, nucleoli and other extremely small structures. An absolute WBC count is critical. Percentages are essentially useless without it. If the absolute number of WBCs is extremely low, there is little utility in trying to determine absolute numbers, as they are all decreased. When using 20x objectives, the number of leukocytes per field is determined using 10 random monolayer fields. This average number is multiplied by 400 and 600 to get a crude range. If using 10x for your low power scan, 100 and 150 should be used to generate a range. Using a 100x objective, the average number of cells per field can be multiplied by 2,000. A 100 cell differential is often adequate for diagnostic purposes; however, a 200 cell differential increases you chance of seeing pathologic changes and getting a more representative sample.
Segmented neutrophils normally have five lobes. Any more and it is considered hypersegmented, indicating senescence. Smooth blue to pink cytoplasm.
Two segmented neutrophils and a monocyte in a dog.
Figure 4
Band neutrophils have no constrictions in the nucleus greater than 50% of the widest part. These are considered an immature form. Metamyelocytes have a kidney shaped nucleus with a mild indentation and are slightly larger than band neutrophils. They are even more immature than band neutrophils and should not normally be seen in circulation. Myelocytes are generally the most immature neutrophil seen in circulation and have a round nucleus, with a chromatin pattern similar to the others in the neutrophil line, only less intensely staining. A left shifts is when there is an increase in immature neutrophils and indicates non-specific inflammation / demand for neutrophils.


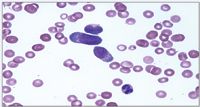
Figure 4
A regenerative left shift is when the total number of immature forms is increased, but still less than the total number of segmented neutrophils. A degenerative left shift is when the total number of immature forms outnumbers the segmented neutrophils. This indicates that the bone marrow cannot keep up with demand and thus has resorted to releasing more and more immature forms. Toxicity is another key feature that must be assessed. Toxicity is the morphologic changes seen that occur when production of neutrophils is markedly increased or when endotoxin is present. Döhle bodies represent the first sign of toxicity. These are blue staining inclusions in the cytoplasm, often either at the periphery or near the nucleus.
Band neutrophil with several blue Döhle bodies
Figure 5
The next stage of toxicity is blue and foamy cytoplasm. Both must be present to be considered the second level of toxicity. Toxic granulation consists of fine pink granules in the cytoplasm represent the most severe toxic change. This toxicity is rarely seen in small animals. This change should be accompanied by prominent examples of the first two stages of toxicity. Monocytes are larger than neutrophils with blue, often smooth cytoplasm, +/- discrete vacuoles. Their pleomorphic nucleus ranges in shape from ovoid to segmented/lobulated (most common). Their nucleus is wider and stains less intensely than neutrophils. They can be confused with toxic immature neutrophils, except monocytes don't get Döhle bodies. Eosinophils have a segmented nucleus and overall size that is similar to neutrophils. Round vivid pink granules in dogs and more rod-shaped granules in cats fill the cytoplasm. Mature lymphocytes are roughly 1.5 to 2 times the size of a red cell, have an evenly stippled, grainy chromatin pattern and a uniformly high N:C ratio. They will get larger as they are less mature. Reactive lymphocytes / plasmacytoid cells / immunocytes are slightly larger than a normal mature lymphocyte more cytoplasm, which is often royal blue, save around the nucleus, indicate a non-specific antigenic stimulus. Atypical lymphocytes include a feature that is not completely normal such as a pleomorphic (notched, oblong, cleaved, multiple, etc.) nucleus or vacuolated cytoplasm. Their significance is speculative. Lymphoblasts are generally 20µm or greater, have a clumped, poorly staining chromatin and one or more prominent nucleolus. Large Granular Lymphocytes (LGL) are larger than normal mature lymphocytes, have more cytoplasm, which tends to be pale blue to almost clear and may or may not contain a few pink to purple granules in the cytoplasm.


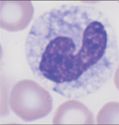
Figure 5
Figure 6


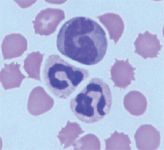
Figure 6
Newsletter
From exam room tips to practice management insights, get trusted veterinary news delivered straight to your inbox—subscribe to dvm360.













Podcast CE: A Surgeon’s Perspective on Current Trends for the Management of Osteoarthritis, Part 1
May 17th 2024David L. Dycus, DVM, MS, CCRP, DACVS joins Adam Christman, DVM, MBA, to discuss a proactive approach to the diagnosis of osteoarthritis and the best tools for general practice.
Listen



