Urethral obstruction in cats: Catheters and complications (Proceedings)
Using proper technique and catheters minimizes post-obstructive inflammation in cats.
• Using proper technique and catheters minimizes post-obstructive inflammation in cats.
• Cats with urethral obstruction may develop complications due to metabolic or urethral issues.
• When necessary, soft indwelling catheters are left in place until metabolic derangements are corrected, the urine clears and the cat is likely to void normally.
• Post-obstructive diuresis is common and can lead to significant fluid and electrolyte losses.
• Difficulty voiding is common post-obstruction and may be due to reobstruction, urethral spasm or bladder atony.
Pathophysiology
The most common causes of voiding disorders in cats include: obstruction with urethral plug, urolith, or blood clot; urethrospasm resulting in functional obstruction (usually post blockage); bladder dysfunction (detrusor atony) following blockage; and neurologic lesions leading to detrusor atony. Other causes include urethral stricture, neoplasia of the bladder neck or urethra, and extraluminal obstruction.
With lower urinary tract obstruction, the urinary bladder distends beyond its usual accommodating size. As intravesicular pressure increases to threshold levels, stretch receptors are activated and afferent information is relayed to higher centers. In an animal with an intact neurological system, these messages will trigger attempts to void. In an animal who cannot eliminate urine, the increased intravesicular pressure continues to build and is transmitted "upstream" to the ureter and ultimately to the kidney. Increased intratubular pressure opposes the forces driving glomerular filtration; ultimately RBF and GFR decline. Tubular concentrating ability and other tubular functions are also affected, leading to impaired sodium and water reabsorption, and impaired excretion of acids and potassium. Uremia, acidosis, hyperkalemia and volume depletion result. Inflammatory cells infiltrate urinary tract tissue and over time, mucosal damage or primary renal failure may occur. Acute complete urinary obstruction causes uremia within 24 to 48 hours and death within 60 – 75 hours. Following relief of obstruction, renal tubular impairment continues for some time, presumably to resolve the dramatic water and electrolyte aberrations that have developed. Renal tubular damage or overall nephron loss also contributes to the dramatic polyuria observed post-obstruction.
Diagnostic Approach to Micturition Disorders in Cats
The diagnostic approach includes a problem-specific history and a physical examination that includes neurological evaluation (especially tail and anal tone, perineal sensation and hindlimb function). In addition, observation of voiding is important to determine how the animal postures, quality of urine stream, bladder expressibility, and whether the bladder is emptied fully after voiding. Observation of voiding can be difficult in cats in the hospital, so a detailed client history is imperative. A urinalysis is recommended to rule out iatrogenic or secondary UTI. Other components of a minimum data base (CBC, biochemical panel) can be selected based on the cat's general condition and history.
Imaging with survey radiography is recommended in all cases because urolithiasis is fairly common in cats. Ultrasonography can be more sensitive for the detection of small uroliths or soft tissue masses in the urinary tract. Small uroliths can move back and forth between the urinary bladder and urethra, making their detection more difficult. Excretory urography or contrast cystourethrography may be indicated to rule out or characterize anatomical abnormalities in young cats, to completely rule out anatomical obstruction, or following traumatic injuries or surgery. Additional imaging procedures may be necessary to rule out or characterize spinal lesions. Cystoscopy is increasingly applied in order to visualize the urinary bladder and urethra and may help confirm small uroliths or inflammatory/neoplastic lesions. In female cats, rigid cystoscopy allows good visualization of the urinary bladder and urethra and introduction of biopsy or other instruments. Small flexible or semi-flexible scopes are required in male cats, however, and offer limited visualization and instrumentation options.
Often, transurethral urinary catheterization is used to rule in/out mechanical obstruction, because catheterization will be difficult or "rough" at the obstructed site. If a catheter advances quite easily, the obstruction may be functional rather than anatomical. However, a flexible catheter may be passed retrograde through an incomplete intraluminal or extraluminal obstruction fairly easily (especially soft tissue masses) while spontaneous antegrade voiding remains difficult or impossible for the animal.
In rare cases, specialized urodynamic tests that evaluate lower urinary tract function are used to further characterize a micturition disorder. Urethral pressure profiles are occasionally used to document urethrospasm or to pinpoint focal obstruction. These tests are available at some referral teaching hospitals and are more commonly performed in cats in research settings. Urodynamic testing can clarify dysfunction in complex cases, congenital incontinence, or cases that fail to respond to treatment.
Management of Urethral Obstruction
Key principles
Manage fluid and electrolyte needs in acute complete obstruction (uremia, dehydration, hyperkalemia): Fluid therapy must be initiated to meet acute volume needs (body weight in kg x percent dehydration = L deficit, usually 200-400 mls in 80 – 100 ml boluses) and given over 2 – 3 hours. An ECG and electrolyte measurements should be performed to assess serum potassium. Sodium bicarbonate (if moderately hyperkalemic, acidotic) or calcium gluconate (if severely hyperkalemic or arrhythmic) can be administered for short term relief of hyperkalemia while the urinary obstruction is removed. Calcium gluconate is also appropriate for the cat with significant ionized hypocalcemia. Maintenance fluid and bicarbonate needs will depend on urine output and severity of acidosis.
Alleviate or bypass urethral obstruction immediately:
• Urethral catheterization: For obstructed cats, sterile polypropylene catheters or rigid olive tip catheters are often used initially. Other, less traumatic, soft catheters are available, some with tiny wire stylets to ease passage. An advantage of longer, soft catheters is their suitability as indwelling catheters, if needed. In general, well- lubricated smaller catheters should be chosen to be as atraumatic as possible. The catheter tip is advanced to the point of obstruction, and sterile saline or other non-glucose crystalloid should be used to copiously flush the urethra. Using an extension line and a 10 ml syringe for flushing helps maximize flow and return. The catheter is pulled back when there is resistance to flow, then advanced again if possible. The goal is to dislodge and flush the obstructing material antegrade, out the tip of the urethra. If the bladder is full, very gentle attempts at expression can help expel a plug at this point. If flushing is minimally successful, the external urethral orifice can be held closed, and additional gentle flushing used to attempt to dilate the urethra and retropulse debris or small uroliths back into the urinary bladder. Following retropulsion of uroliths, the uroliths are removed via cystotomy to prevent recurrent obstruction. (Voiding hydropropulsion, useful for removing uroliths smaller than the urethral lumen, usually is not advised in patients that have already become obstructed, because it is known that a urolith larger than the urethra is present.) The bladder should be flushed copiously to eliminate remaining inflammatory and crystalline material.
• Tips for difficult catheterizations:
o Adequate sedation and restraint is key.
o If catheterization is difficult, cystocentesis can be used for temporary decompression; reducing the back pressure in the urinary by cystocentesis may also facilitate flushing and catheterization. Cystocentesis is not advised if the obstruction is known to be prolonged, or if the urine is extremely bloody/port wine in color, suggesting devitalized bladder wall. To avoid excessive bladder wall trauma, use a small gauge needle attached to an extension tube
o Use of general anesthesia or smooth muscle relaxants (prazosin or acepromazine) may help in the more challenging cases.
Plan for longer term needs, including 1) assessing the entire urinary tract for uroliths or multiple lesions; 2) providing for long term relief or correction of a persistent obstruction; 3) reduce the likelihood of reobstruction and anticipate post-obstruction issues (below). In cats with the first episode of obstruction, a urinalysis and survey radiographs are indicated. In cats with recurrent episodes, additional imaging with ultrasonography and contrast techniques may be indicated.
Post Obstructive Issues
• Indwelling urethral catheters: With acute, easily removed urethral plugs, an indwelling catheter is unlikely to be necessary. Indwelling catheters are indicated to prevent reobstruction 1) in cases of difficult catheterization where significant urethral trauma has occurred, 2) when large amounts of crystalline debris remain even after bladder flushing, 3) in severely ill cats with metabolic compromise. Indwelling catheters also are used to monitor urine output and to manage detrusor atony or functional obstruction. Non-irritating 5Fr red rubber catheters or infant feeding tubes are preferred. All urinary catheters can be considered irritating to the urethra, which can worsen inflammation or urethrospasm, but this disadvantage must be weighed against the probability of reobstruction, multiple catheterizations, and additional client cost or frustration.
• Indwelling catheters are left in place 24 – 72 hours depending on the individual circumstances. When the urine flowing is fairly clear of crystalline debris, haziness and blood, the catheter is removed. The cat is monitored during the day to ensure he can void normally.
• Ins and outs: Post-obstructive diuresis can lead to remarkable amounts of fluid loss (may exceed 2 liters/day). Tailoring the fluid administered "in" to meet the urine coming "out" helps clinicians meet variable fluid needs for the first couple of days. In this situation, insensible fluid needs can be calculated at 10 – 20 ml/kg/day, and then urine volume measured and replaced as measured. Over time, fluids will need to be slowly tailored so that the animal can be weaned off fluid therapy. Most cats will need potassium supplementation during the post-obstructive diuresis.
• Urethrospasm is a challenging complication of feline obstruction. Short term administration of smooth muscle relaxants (prazosin), striated muscle relaxants (diazepam) and/or analgesics (NSAIDs, Opioids) are minimally helpful. Diazepam may transiently aid bladder expression in some cats. All of these drugs have potential adverse effects as well. "Tincture of time" is the most reliable treatment for urethrospasm; however the urinary bladder must be kept small with urinary catheterization or gentle manual expression in the meantime.
• Detrusor atony is also possible following urinary obstruction and bladder overdistension. A cat whose bladder remains larger than a golf ball following a voiding attempt may require placement of an indwelling catheter for a variable period of time (usually 1-3 days) to maintain a small bladder size. Recovery of normal detrusor function will be enhanced by preventing excessive detrusor stretch or strain in the days following relief of the obstruction.ing. Atony can be managed with manual bladder expression if urethral resistance is low and expression is not difficult or painful. Manual expression of urine, especially in the face of any increased outlet resistance, can create further bladder wall trauma and may delay return to normal function. Bethanechol can also be useful in the recovery of acute detrusor atony,: however urethral outlet resistance must be lowered (typically with pharmacologic means) before introducing bethanechol.
• Urinary tract infection: Iatrogenic infection is common after alleviating lower urinary tract obstruction, or after prolonged urine retention. Ideally, antimicrobials (chosen based on urine culture and susceptibility) are withheld until the urinary catheter has been removed and the animal is urinating adequately. However, if signs of fever, renal pain, or sepsis are evident, urine should be cultured and antimicrobials administered immediately.
• Urethral tear or rupture: With proper technique, urethral damage is unlikely during urinary catheterization. Partial tears or ruptures can be confirmed by urethrography and usually are managed with an indwelling urinary catheter or cystostomy tube placement.
• Perineal urethrostomy is avoided during acute obstructive episodes except as a salvage procedure.
Tips for Preventing Catheter Complications
• Leave only soft, non-irritating catheters such as silicone or Teflon catheters or soft infant feeding tubes in the urethra. Tomcat catheters (polypropylene) are extremely irritating when left in contact with the urethral mucosa, and are more likely than softer catheters to cause bladder trauma when left indwelling. When using an indwelling urinary catheter, always use a closed collection system to decrease the odds of ascending bacterial infection.
• Consider the use of a urethral relaxant during and after the period of catheterization. See Table 1 for medications and doses.
• Consider the one-time use of a nonsteroidal anti-inflammatory such as ketoprofen at the time of catheterization. This may be contraindicated in animals where renal azotemia is suspected or confirmed.
• Ensure patency of the indwelling catheter at all times and monitor urine output. The bladder should not distend at all while the catheter is in place.
• Consider the use of anxiolytic and/or mildly tranquilizing medication during and immediately after the period of indwelling catheterization. See Table 1 for medications and doses. These medications may reduce straining and sympathetic tone resulting from stress. Although amitryptyline has been described to promote urethral relaxation and propulsion of urethral plugs in cats, and offers slightly earlier relief of hematuria and straining in non-obstructed cats, its use in acute situations may increase the likelihood of urine retention and early recurrence of bladder inflammation in cats.
The prognosis for voiding disorders in cats depends on the initiating cause and the duration of dysfunction. Most cats with post-obstructive voiding difficulty will improve with time and proper management. Several days to a week may be necessary before normal voiding returns. With reversible neurologic lesions, return of urinary function usually accompanies recovery of other motor functions; however, pharmacologic treatments may be required during the recovery time period. Medical treatments are usually continued for several days after voiding function has returned, then tapered. Cats with chronic or irreversible neurologic lesions may not improve significantly with treatment, or may require lifelong management. Surgical salvage (urethrostomy) may be necessary in cases of permanent urethral damage.
Long term preventive care should be initiatied for cats following urethral obstruction.For cats with struvite crystalluria or mineralized plugs, struvite preventative dietary management can be used. Uroliths should be analyzed quantitatively (most are calcium oxalate) and preventive strategies applied according to mineral composition. Cats with non-crystalline, inflammatory plugs should be managed as for idiopathic cystitis. Owners should be advised of the high likelihood of recurrence for any of these etiologies.


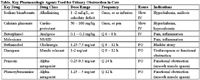
Table. Key Pharmacologic Agents Used for Urinary Obstruction in Cats
References
Bartges JW (1996), "Pathophysiology of urethral obstruction," Vet Clin North Am Small Anim Pract 26:255-64.
Lane IF (2000), "Diagnosis and management of urinary retention," Vet Clin North Am Small Anim Pract 30:25-57.
Lees GE (1994) " Management of voiding disability following relief of urethral obstruction," in John August, ed, Consultations in Feline Internal Medicine, 2nd ed. Philadelphia, WB Saunders.
Olby N, (2006), "Neurogenic micturition disorders," in John August, ed, Consultations in Feline Internal Medicine, 5th ed, Philadelphia, Elsevier.
Fischer JR, Lane IF (2007). Incontinence and urine retention. In Elliott and Grauer, eds. BSAVA Manual of Canine and Feline Nephrology and Urology, 2nd ed.
Drobatz, K. (2008) Emergency management of the critically ill cat with urethral obstruction. In Bonagura and Twedt, eds, Kirk's Current Veterinary Therapy XIV.
Achar et al (2003). Amitriptyline eliminated calculi through urinary tract smooth muscle relaxation. Kidney Int 64:1356.














