The importance of a five-part differential leukocyte count
Advancements in hematology have aided veterinarians greatly. Today's equipment for inclinic hematology analysis can provide accurate white blood cell (WBC) counts and partial or complete differential leukocyte counts. When considering leukocyte differentials, practitioners may ask whether a five-part differential is necessary. In a word, yes. To interpret leukocyte changes in a patient accurately, practitioners must obtain a WBC count and a complete fivepart differential. They should also obtain a peripheral blood film to assess the leukocytes for any morphologic changes. In some cases, practitioners may need to do serial complete blood counts (CBCs) to understand the changes in the different leukocyte forms during various disease states.
Advancements in hematology have aided veterinarians greatly. Today's equipment for inclinic hematology analysis can provide accurate white blood cell (WBC) counts and partial or complete differential leukocyte counts. When considering leukocyte differentials, practitioners may ask whether a five-part differential is necessary. In a word, yes. To interpret leukocyte changes in a patient accurately, practitioners must obtain a WBC count and a complete fivepart differential. They should also obtain a peripheral blood film to assess the leukocytes for any morphologic changes. In some cases, practitioners may need to do serial complete blood counts (CBCs) to understand the changes in the different leukocyte forms during various disease states.
Five parts equal more insight
WBC counts may give practitioners some insight into the severity of changes within the leukocytes; however, the absolute number of all five leukocyte types can help practitioners pinpoint the animal's problem. Some of the more common leukocyte abnormalities are due to inflammatory disease, glucocorticoid influence (i.e., stress), and epinephrine influence (i.e., excitement).
In addition, practitioners can categorize types of inflammatory disease by assessing the degree of change in each leukocyte and identifying the morphologic changes in the peripheral blood film. Morphologic changes include the presence of immature neutrophils (i.e., left shift), toxic neutrophils, and reactive lymphocytes ( Figures 1-3). These changes, which cannot be identified by hematology analyzers in clinics or reference laboratories, may be the only indication for the presence of inflammatory disease.



Figure1. A normal, mature neutrophil with relatively clear, pale-blue-staining cytoplasm is next to the larger normal monocyte with moderate amounts of blue cytoplasm and cytoplasmic vacuoles.
Characterizing a leukogram requires pattern recognition. Table 1 lists several common patterns indicated by quantitative leukocyte disturbances.
As you can see, the table uses arrows—not absolute numbers—because the pattern of change is more important than a specific number. Despite this, neutrophil number guidelines can be helpful in interpreting leukograms. For example, note the overlap in the three basic leukogram patterns (i.e., inflammation, stress, and excitement).In each of these scenarios, a neutrophil increase is possible, but the neutrophilia is rarely higher than 15,000/µl to 20,000/µl with excitement and typically less than 30,000/µl with stress.


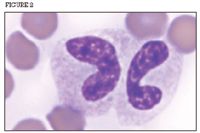
Figure 2. Two immature (band) neutrophil forms with mild to moderate toxicity based on the moderate, blue-staining cytoplasm and slight foamy appearance of the cytoplasm.
What the changes mean
Increases and decreases in each leukocyte type indicate different things.
Neutrophils. Increases can occur with inflammatory disease, stress, and excitement. Because neutrophils are the body's first line of defense, neutrophil changes are commonly seen in a variety of inflammatory diseases caused by infectious and noninfectious sources. Neutrophils may also decrease with inflammation if the inflammatory process is severe or overwhelms the bone marrow.
In cases of inflammation and neutrophilia with superimposed glucocorticoid or epinephrine influences, the presence of immature or toxic neutrophils may be a practitioner's only means of identifying a concomitant inflammatory process.
Lymphocytes. Lymphocytes are components of the immune system. In dogs, lymphocyte increases that are not associated with a neoplastic lymphocytosis typically stem from systemic, antigenic stimulation caused by infectious or noninfectious sources.
In excited cats, lymphocytosis may occur because of lymphocyte redistribution. Lymphocytosis in excited cats can easily reach 20,000/µl. A decrease in lymphocyte numbers may be seen with various conditions; however, it is most commonly seen when there is a glucocorticoid influence.


Figure 3. A toxic band neutrophil with two Döhle bodies (arrowheads).
Monocytes. Monocytes are precursors to tissue macrophages. Monocytosis typically indicates a peripheral demand for macrophages, which can clean up tissue debris and help fight selected infectious diseases such as fungal or mycobacterium infections.
Eosinophils and basophils. Increases in these granulocytes are commonly found in selected parasitic infections, hypersensitivity responses, and allergic phenomena. Eosinophils may decrease in the glucocorticoid-influenced leukogram.


Table 1: Commonly Encountered Leukocyte Profiles and Their Potential Differential Patterns
Manual vs. automated
As stated previously, interpreting leukocyte changes accurately requires separating all five leukocyte types. Most in-clinic hematology analyzers available today provide only a twoor three-part differential automatically, printing a report for all the granulocytes (neutrophils, eosinophils, and basophils), plus the lymphocytes and monocytes (which the analyzer may also combine). A complete five-part differential must be determined manually in these situations.
In addition, an analyzer that reports a differential may not accurately separate the different leukocytes. Many analyzers, particularly the impedance counters that check only the volume and number of particles, may not be able to correctly distinguish small clumps of platelets and nucleated red blood cells. Platelet clumps can be misclassified as leukocytes or erythrocytes, and nucleated red blood cells can be misclassified as leukocytes or, specifically, lymphocytes. Furthermore, large or unidentifiable atypical cells, toxic immature neutrophils, and markedly reactive lymphocytes can also be misclassified.
To obtain a complete, five-part leukocyte differential and distinguish blood-formed elements better, reference laboratories use more advanced analyzers (either laser flow cytometry or enzyme cytochemistry) with more than simple impedance technology. In recent years, manufacturers have incorporated laser flow cytometry into analyzers for in-clinic use. These analyzers, such as the LaserCyte® (IDEXX Laboratories), provide blood analyses that are similar to those obtained by reference laboratories. Even in reference laboratories,however, microscopic evaluation of the peripheral blood film is essential. Practitioners should consider a blood film evaluation as a routine component of every CBC
In summary, the best way to obtain rapid, reliable hematology information involves two steps: Using an in-clinic analyzer that provides precise and accurate numerical data—including a five-part leukocyte differential—and conducting a brief microscopic evaluation of a peripheral blood film. This two-part analysis is essential for identifying and managing various diseases.















