Leptospirosis: New Tests Improve Diagnostic Capabilities
Recent developments in serologic testing offer new insight into this zoonotic disease.



Leptospirosis is a complicated disease for a variety of reasons. Clinical presentations can vary, disease-causing serovars can be difficult to pin down, and the zoonotic potential can threaten both veterinary caregivers and pet owners.
Diagnosis is another aspect of this disease that continues to challenge veterinary professionals. The microscopic agglutination test (MAT) has long been considered the preferred diagnostic method, but it has many shortcomings. Fortunately, recent developments in serologic testing may help to improve our diagnostic capabilities, which can translate into earlier intervention and improved patient outcomes.
Overview of Diagnostic Options
Once exposure and infection occur in a dog, leptospires multiply in the bloodstream for about 4 to 10 days before spreading into body tissues such as the kidneys, liver, eyes, and central nervous system. At this point, they replicate in the renal tubules, facilitating urine shedding within 10 to 14 days. This timeline is important for understanding what serologic tests and other diagnostic modalities actually detect.
Some serologic tests rely on identifying immunoglobulin (Ig)M and IgG antibodies produced in response to the infection. IgM antibodies are generated relatively early—within 3 to 10 days of infection—but they don’t persist for very long, tending to decline by approximately 14 days. IgG antibodies rise
more slowly, appearing 2 to 3 weeks post infection, but IgG levels remain elevated for a longer time.
Specific diagnostic tests for leptospirosis generally can be divided into 2 types:
- Tests that identify the organism itself (eg, culture testing, polymerase chain reaction [PCR] testing)
- Tests that detect the body’s immunologic response to the organism, such as the MAT or enzyme-linked immunosorbent assay (ELISA)
Test results must be interpreted in context. For example, titers take time to rise, so certain types may be low or negative during the very early stages of disease. Similarly, dogs that are vaccinated against leptospirosis are expected to have detectable antibodies, so a titer should be evaluated in light of the
pet’s vaccination history.
Point-of-care tests that facilitate rapid and accurate diagnosis of leptospirosis are also available (eg, from IDEXX Laboratories and Zoetis). These tests have several advantages, including high sensitivity, small blood sample size, and quick results that permit early intervention for the patient and implementation of safety precautions for the owner to help reduce the likelihood of zoonotic transmission. Because administration of antibiotics can affect many diagnostic tests for leptospirosis (including PCR and MAT), some diagnostic algorithms recommend first obtaining blood and urine samples. In many cases, veterinarians make a tentative diagnosis of leptospirosis based on clinical signs, suspicious chemistry panel/complete blood count (CBC) results, a medical history that supports the possibility of exposure, and supportive results from MAT testing. These results can all be inconclusive,
however, making more sensitive testing modalities critically important.
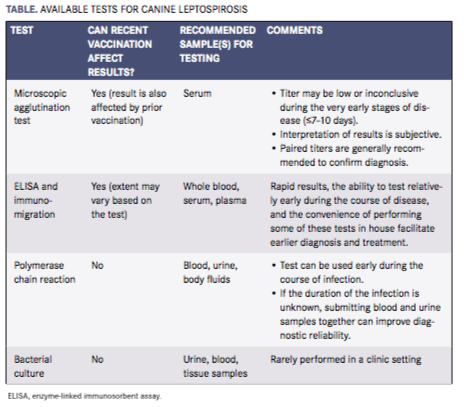
The Table summarizes the available tests for leptospirosis. As described here, all the tests have advantages and disadvantages, and many diagnostic algorithms recommend combining tests to improve diagnostic accuracy.


Microscopic Agglutination Test
The MAT is likely the most widely used test for the diagnosis of leptospirosis. Relatively inexpensive and performed on serum at a diagnostic laboratory, the test involves creating serial dilutions of the patient’s serum and exposing each dilution to live leptospires grown at the laboratory. Agglutination is determined via dark-field microscopy such that the highest serumdilution that causes at least 50% of the leptospires in the sample to agglutinate is considered the patient’s titer.
Most diagnostic laboratories that conduct MAT titers maintain quantities of leptospirosis serovars based on the serovars that occur locally or in the patient’s species, but cross-reactivity can occur. Therefore, the serovar that has the highest titer does not necessarily represent the serovar causing infection in
a specific patient.
False-negative results or very low titers are possible during the early stages of illness (eg, during the initial 7—10 days) if antibiotics have been initiated prior to testing or if the serovar causing the infection is not included among the serovars used to conduct the test. False-positive results can occur in recently vaccinated patients.
In an unvaccinated patient with suspicious clinical signs and chemistry/CBC findings, a single high MAT titer is consistent with leptospirosis infection. However, titers in vaccinated dogs can be quite high, and a high titer in a vaccinated dog displaying clinical signs is not necessarily due to infection with leptospirosis. If the initial titer is inconclusive, however, a convalescent titer is recommended 2 to 4 weeks later. Ideally, a 4-fold or greater change (normally an increase) in titer strongly supports a diagnosis of leptospirosis. However, antibiotics can blunt the convalescent titer.
Point-of-Care Assays and Elisa Tests
Because of some of the shortcomings of the MAT, ELISA tests and other point-of-care tests have been developed. ELISA tests generally detect IgG and/or IgM antibodies to leptospires. Because IgM antibody levels increase relatively quickly before waning, ELISA tests that detect IgM can be helpful during the
early course of illness, when MAT is more likely to be negative. A recently released immunomigration test (WITNESS Lepto, Zoetis) detects IgM antibodies as early as 4 days post infection but is somewhat different from an ELISA test (although the functionality is arguably similar). Serum IgG levels tend to
increase 14 to 21 days after infection and peak within 30 days. Some ELISA tests detect both IgG and IgM, which increases the likelihood of disease detection.
Leptospira possess outer surface proteins that can induce an immune response in infected dogs. Some ELISA tests can detect antibodies to these proteins. For example, IDEXX Laboratories’ SNAP Lepto Test (an ELISA test) detects antibodies to lipoprotein LipL32, which occurs abundantly on the outer membrane of Leptospira bacteria. Both of these tests provide rapid results, and the ability to conduct
the tests relatively early during the course of disease offers additional clinical advantages. However, both tests may yield positive results in dogs recently vaccinated against leptospirosis, so results should be interpreted in light of vaccine history.
Polymerase Chain Reaction
PCR detects the DNA of leptospires in a specimen. The test can be conducted on blood samples, ideally within the first 10 days after infection. After approximately 14 days, the organism is more likely to have invaded the renal tubules, so urine should be submitted. Submitting blood and urine samples together can improve diagnostic reliability, especially when the time of exposure is undetermined. Some test protocol algorithms recommend performing PCR testing and serology (eg, ELISA) together to improve diagnostic reliability. Other body fluids, such asaqueous humor and cerebrospinal fluid, may also be acceptable for PCR testing. Subclinical leptospirosis carriers may test positive using PCR testing.
Potential advantages of PCR testing include the ability to conduct the test fairly early during the course of disease and the fact that recent vaccination does not influence results. Recent administration of antibiotics or a low quantity of leptospires in the sample may, however, produce false-negative results.
And, although a positive PCR result confirms the diagnosis, a negative result does not rule it out. Recent administration of antibiotics or a low quantity of leptospires in the sample may result in false-negative results.
Bacterial Culture
Culture testing can be performed on urine, tissue samples, or blood, which ideally should be obtained before antibiotics are administered. Because leptospires remain in the blood for only a short time, blood cultures are recommended during the first 10 days of infection and urine samples later in the course of disease.
Outside a research setting, cultures are not widely used because the leptospirosis organisms do not survive transportation well and a special culture medium is required to maintain them. Also, the organisms grow very slowly, so results take several weeks, which would delay treatment and protective measures in a clinic setting. Further, leptospires can be cultured from blood or urine samples in clinically healthy animals, so culture results can be difficult to interpret in a practice setting.
Dr. Karen Todd-Jenkins received her VMD degree from the University of Pennsylvania School of Veterinary Medicine. She is a medical writer and has remained in clinical practice for over 20 years. She is a member of the American Medical Writers Association and One Health Initiative.
Recommended Reading:
- Goldstein RE. Leptospirosis: Risk from a clinical perspective. Proc NAVC. 2017;523-525.
- Greene CE, Sykes JE, Moore GE, et al. Leptospirosis. In Greene CE (Ed): Infectious Diseases of the Dog and Cat, ed 4. St. Louis: Elsevier Saunders; 2012:431-446.
- IDEXX Laboratories. Package insert: Canine Leptospira Antibody Test Kit (SNAP). Idexx website: idexx.com/resource-library/smallanimal/snap-lepto-product-insert-en.pdf. Published 2015. Accessed May 2, 2017.
- IDEXX Laboratories. The in-house SNAP Lepto Test and the Leptospira ELISA at IDEXX Reference Laboratories. Idexx website: idexx.com/files/small-animal-health/products-and-services/reference-laboratories/dxupdate-snap-lepto-labs-elisa.pdf. Published July 2015. Accessed May 2, 2017.
- Lunn KF. Leptospirosis. In Bonagura JD, Twedt DC (Eds): Kirk’s Current Veterinary Therapy XV. St. Louis, MO: Elsevier Saunders; 2014:1286-1289.
- McDonough PL. Leptospirosis. In Tilley LP, Smith FWK (Eds): Blackwell’s Five Minute Veterinary Consult, ed 6. Ames, IA: Wiley Blackwell; 2016;798-789.
- Sykes JE, Hartmann K, Lunn KF, et al. 2010 ACVIM small animal consensus statement on leptospirosis: diagnosis, epidemiology, treatment and prevention. J Vet Intern Med. 2011;25:1-13.
- Weese JS, Fulford MB. Bacterial diseases: Leptospira spp. In Weese JS, Fulford MB (Eds): Companion Animal Zoonosis. Ames, IA: Wiley Blackwell; 201:157-164.
- Winzelberg S, Tasse SM, Goldstein RE, et al. Evaluation of SNAP® Lepto in the diagnosis of leptospirosis infections in dogs: twenty two clinical cases. Int J Appl Res Vet Med, 2015;13(3):193-198.
















