Oncology myths, part 2
Experts separate fact from fiction
In case you missed it, check out part 1 of oncology myths.
Myth 1: Initial diagnosis of malignant mammary mass does not predict development of a second malignant mass.
Contrary to the “canine 50/50 rule,” which says mammary masses in dogs will be benign half the time, a study by Stratmann et al, in Veterinary Surgery in 2008, of 99 female dogs revealed that only 26% of their masses were benign, while 74% were malignant.1
Adenomas were the most common type of benign mass and carcinoma the most common malignant mass. All masses were completely excised with clean histopathologic margins using local or regional mastectomies. Fifty-seven patients (58%) developed a new mammary tumor following initial local and regional mastectomy in one of the remaining ipsilateral mammary glands. Dogs with an initial malignant tumor were more likely to develop another malignant tumor. Time from first surgery to development of a new mass was 1 to 60 months. The authors concluded that this information should be taken into account when deciding on radical vs regional mastectomy.1
As a reminder, the risk of developing canine mammary cancer is 0.5% if spayed before the first heat cycle, 8% after the first heat cycle, and 26% after the second heat cycle.2
Myth 2: Disagreement between cutaneous cytology and subcutaneous histopathology as to samples classified as noncancerous is less than 10%.
In a study by Ghisleni et al, 67 of 292 cytology samples were classified as noncancerous. Of the 67 cases, there was agreement between cytology and histopathology (true negative) in 46 (68.7%). There was a false negative diagnosis of cancer on cytology in 21 of 67 samples (31.3%), meaning that cancer was present but not diagnosed.3
As a reminder:
- Sensitivity = true positive/false negative
- Specificity = true negative rate/false positive


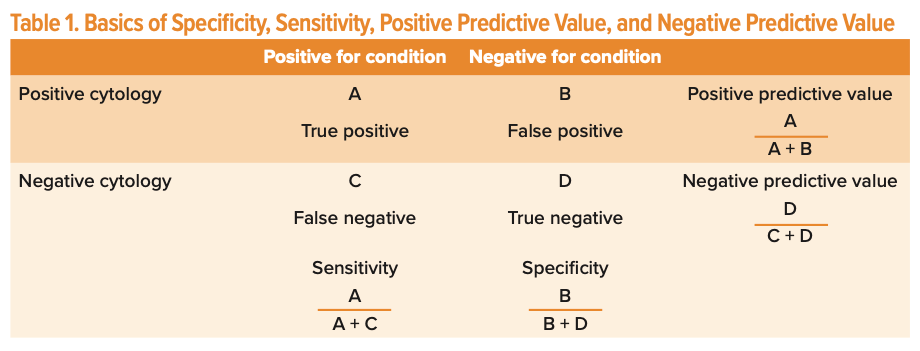
Of the 292 samples, 176 were diagnosed as cancer on cytology and 175 of 176 were confirmed on histopathology (high true positive for malignant diagnosis). No benign cytologic samples were reclassified as malignant on histopathology (high true positive for benign diagnosis).3
And of those 292 samples, 49 (16.8%) were excluded because of poor cellularity. Thus, slides should be assessed before submission for good cell quality to reduce rejection secondary to low cellularity, cell degeneration, hemodilution, and/or artifacts.3
Helpful tips for the general practitioner
1. If the tissue specimen is softer, a smaller needle and syringe will be more effective at preventing cores from forming and thus decreasing the chance of blood contamination.
2. If the tissue is firm, a larger needle and syringe can be used to create enough negative pressure to draw cells into the needle.
3. When redirecting the needle, it should not transcend beyond the mass because the cells can be displaced in the barrel of the syringe and not expelled onto the slide. In addition, if the needle goes beyond the mass, contamination by infected or neoplastic cells can transcend a tissue plane and affect future surgery.
4. The needle should be directed as perpendicularly as possible to a subcutaneous or skin mass so that the needle tract is removed during subsequent surgery.
5. Negative pressure should not be applied for more than a few seconds. Prolonged negative pressure can cause damage to cells, aspiration into the barrel, and disruption of the blood vessel.
6. Inadequate negative pressure or slow and/or shallow needle passages can lead to poor cellularity.
Other tips and tricks
1. Use a new needle for each mass to be aspirated.


Topography diagrams by Mary Deatherage
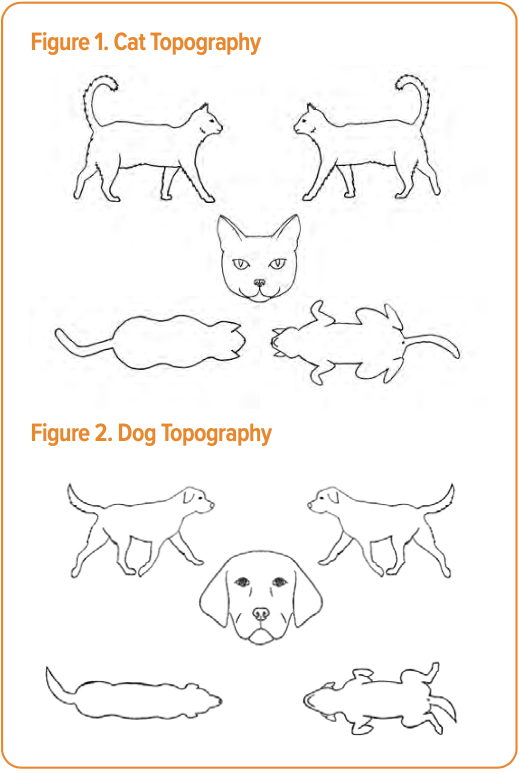
2. Topography sheets are useful for documenting location (Figures 1 and 2). In addition, the mass should be measured with calipers in 3 dimensions and recorded on the sheet. This allows objective assessment of growth.
- If the mass is on a leg or the body, number cm proximal to distal x number cm medial to lateral x number cm deep.
- If the mass is on the head, number cm rostral to caudal x number cm medial to lateral x number cm deep.
- Calipers should be used consistently with care, not to “squeeze” a mass and give a false representation of the mass as being smaller than it actually is.
Owner education
1. False negatives can occur (about 31%) but false positives are rare. Thus, if a good answer (ie, no cancer) is achieved, but the mass is not behaving as benign, a tissue sample for confirmation is recommended.4
2. Cytology does not give a grade for cancer. Histopathology is necessary to provide tumor grade.
3. Cytology is the evaluation of cells. Histopathology is evaluation of tissue.
Myth 3: There is a poorer prognosis for patients with osteosarcoma if preoperative ALP is increased at the time of diagnosis.
This is debatable. In 1998, a study by Ehrhart et al was the first to report the negative prognostic effect on survival time and disease-free interval (DFI) of elevated alkaline phosphatase (ALP) in patients at initial diagnosis.5 This correlation was confirmed in numerous other large meta-analysis studies in veterinary.6 Depending on which study one reads, DFI ranges for elevated ALP at the time of initial diagnosis are 147 to 177 days vs 366 to 546 days for normal ALP at initial diagnosis.6 As in humans, if ALP does not decrease following surgery, the DFI is markedly decreased.5
However, in 2011, Saam et al, published one of the first studies to refute the correlation between an elevated ALP at the time of diagnosis and a poorer prognosis. Several smaller studies followed with the same conclusion. Most of the authors concluded that these results could be secondary to a type II statistical error and/or potentially related to smaller tumor burden. Total serum ALP is a compilation of bone, liver, and steroid isoenzyme values. The authors concluded that an elevated total serum ALP in some dogs with osteosarcoma was secondary to endocrine or liver pathology and that its prognostic reliability in individual dogs was therefore decreased.7
Owner education is essential for patients diagnosed with cancer. Amputation alone has median survival times of less than or equal to 25 weeks, with a 1-year survival of 11.5% and a 2-year survival of 2%.5 Survival times with surgery followed by chemotherapy vary depending on the study and the type of chemotherapeutic, with overall ranges of 1-year survival of 20% to 36.5%, 2-year survival of 18% to 22%, and 3-year survival of 10% to 19%.5,8 Owners of patients with an elevated ALP at the time of initial diagnosis should be provided statistics to guide decision-making and should not proceed with treatment based on this factor alone. An elevated ALP at the time of diagnosis is just 1 potential prognostic factor for this serious bone cancer diagnosis.
Tasha Ostrowski, RVT, graduated from Kansas State University in 2017 with a major in animal sciences and industry, then went on to attend Colby Community College in Colby, Kansas, and became a registered veterinary technician in 2020. Since then, she has been working as a surgery nurse in a multispecialty practice. Her dream is to become a veterinarian and to continue following her passion to care for the animals that bring joy to our lives, no matter their size.
Heather Towle Millard, DVM, MS, DACVS-SA, is a staff surgeon at Phoenix Veterinary Surgical Specialists. With over 15 years of experience, Millard has expertise in advanced soft tissue surgery, oncologic surgery, and general orthopedic surgery. She enjoys mentoring passionate, energetic, and determined young doctors and being part of their journey to success.
References
- Stratmann N, Failing K, Richter A, et al. Mammary tumor recurrence in bitches after regional mastectomy. Vet Surg. 2008;37(1):82-86. doi:10.1111/j.1532-950X.2007.00351.x
- Schneider R, Dorn CR, Taylor DO. Factors influencing canine mammary cancer development and postsurgical survival. J Natl Cancer Inst. 1969;43(6):1249-1261.
- Ghisleni G, Roccabianca P, Ceruti R, et al. Correlation between fine-needle aspiration cytology and histopathology in the evaluation of cutaneous and subcutaneous masses from dogs and cats. Vet Clin Pathol. 2006;35(1):24-30. doi:10.1111/j.1939-165x.2006.tb00084.x
- Cohen M, Bohling MW, Wright JC, et al. Evaluation of sensitivity and specificity of cyto- logic examination: 269 cases (1999-2000). J Am Vet Med Assoc. 2003;222(7):964-967. doi:10.2460/javma.2003.222.964
- Ehrhart N, Dernell WS, Hoffmann WE, et al. Prognostic importance of alkaline phosphatase activity in serum from dogs with appendicular osteosarcoma: 75 cases (1990-1996). J Am Vet Med Assoc. 1998;213(7):1002-1006.
- Bone appendicular OSA. Veterinary Society of Surgical Oncology. Accessed January 6, 2023. https://vsso.org/bone-appendicular-osa
- Saam DE, Liptak JM, Stalker MJ, et al. Predictors of outcome in dogs treated with adjuvant carboplatin for appendicular osteosarcoma: 65 cases (1996-2006). J Am Vet Med Assoc. 2011;238(2):195-206. doi:10.2460/javma.238.2.195
- Phillips B, Powers BE, Dernell WS, et al. Use of single-agent carboplatin as adjuvant or neoadjuvant therapy in conjunction with amputation for appendicular osteosarcoma in dogs. J Am Anim Hosp Assoc. 2009;45(1):33-38. doi:10.5326/0450033















Newsletter
From exam room tips to practice management insights, get trusted veterinary news delivered straight to your inbox—subscribe to dvm360.






")







